Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- 1.WLJ Brachy 3 PDFDokument54 Seiten1.WLJ Brachy 3 PDFmohsinfareed100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- CO2A Sample Question OvaryDokument34 SeitenCO2A Sample Question OvaryAmr MuhammedNoch keine Bewertungen
- 1&2.unsealed Sources Thursday16thMay S JeansDokument119 Seiten1&2.unsealed Sources Thursday16thMay S JeansAmr MuhammedNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- 04 - .Radiation Safety II Brachy Fri - 17th - May - 2013 PCooperDokument27 Seiten04 - .Radiation Safety II Brachy Fri - 17th - May - 2013 PCooperAmr MuhammedNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- 01 - Radiation Protection 1 - WM 2013Dokument42 Seiten01 - Radiation Protection 1 - WM 2013Amr MuhammedNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Systemic Administration of Heparin Ameliorates RadDokument7 SeitenSystemic Administration of Heparin Ameliorates RadAmr MuhammedNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- IMRT & Stereotactic Radiotherapy: Christopher GolbyDokument41 SeitenIMRT & Stereotactic Radiotherapy: Christopher GolbyAmr MuhammedNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- 1.wendy Julian Brachytherapy 1Dokument51 Seiten1.wendy Julian Brachytherapy 1Amr MuhammedNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- 1&2.unsealed Sources Thursday16thMay S JeansDokument119 Seiten1&2.unsealed Sources Thursday16thMay S JeansAmr MuhammedNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- KV Machines, Cobalt Units and Beam Quality: James BeckDokument55 SeitenKV Machines, Cobalt Units and Beam Quality: James BeckAmr MuhammedNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- 1.wendy Julian Brachytherapy 2Dokument50 Seiten1.wendy Julian Brachytherapy 2Amr MuhammedNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Radiotherapy in Practice, Physics For Clinical OncologyDokument276 SeitenRadiotherapy in Practice, Physics For Clinical OncologyAmr Muhammed60% (5)
- 5&6.LinearAccelrators 1314thmay2013 ImranPatelDokument99 Seiten5&6.LinearAccelrators 1314thmay2013 ImranPatelAmr MuhammedNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- RA SourcesDokument1 SeiteRA SourcesAmr MuhammedNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Teletherapy 01Dokument44 SeitenTeletherapy 01Amr MuhammedNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Treatment Planning 04Dokument42 SeitenTreatment Planning 04Amr MuhammedNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Off Budgell FRCR - VerificationDokument46 SeitenOff Budgell FRCR - VerificationAmr MuhammedNoch keine Bewertungen
- Teletherapy 03Dokument28 SeitenTeletherapy 03Amr MuhammedNoch keine Bewertungen
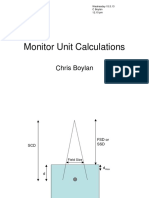
- MU CalculationsDokument17 SeitenMU CalculationsAmr MuhammedNoch keine Bewertungen
- Treatment Planning 01Dokument43 SeitenTreatment Planning 01Amr MuhammedNoch keine Bewertungen
- Imaging & Data Aquasition Michael TrainerDokument96 SeitenImaging & Data Aquasition Michael TrainerAmr MuhammedNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Steve Bolton Photon - InteractionsDokument47 SeitenSteve Bolton Photon - InteractionsAmr MuhammedNoch keine Bewertungen
- Radiation Quantities and Units - Joe Berresford - 13th MayDokument41 SeitenRadiation Quantities and Units - Joe Berresford - 13th MayAmr MuhammedNoch keine Bewertungen
- Treatment Planning 02Dokument56 SeitenTreatment Planning 02Amr MuhammedNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Teletherapy Physics - Session 3: Alan McwilliamDokument31 SeitenTeletherapy Physics - Session 3: Alan McwilliamAmr MuhammedNoch keine Bewertungen
- The Hazard of Accelerated Tumor Clonogen Number Re-Population During Radiotherapy PDFDokument16 SeitenThe Hazard of Accelerated Tumor Clonogen Number Re-Population During Radiotherapy PDFAmr MuhammedNoch keine Bewertungen
- Effect of Surgical Removal On The Growth and Kinetics of Residual TumorDokument6 SeitenEffect of Surgical Removal On The Growth and Kinetics of Residual TumorAmr MuhammedNoch keine Bewertungen
- Co1 Examiners Report - A16Dokument2 SeitenCo1 Examiners Report - A16Amr MuhammedNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Simulation of Yeast Cooperation in 2D: Bulletin of Mathematical Biology March 2016Dokument19 SeitenSimulation of Yeast Cooperation in 2D: Bulletin of Mathematical Biology March 2016Amr MuhammedNoch keine Bewertungen
- Examiners Report - Co1 s17Dokument2 SeitenExaminers Report - Co1 s17Amr MuhammedNoch keine Bewertungen
- Fammthya 000001Dokument87 SeitenFammthya 000001Mohammad NorouzzadehNoch keine Bewertungen
- 1.functional Specification PTP With EDIDokument36 Seiten1.functional Specification PTP With EDIAnil Kumar100% (4)
- Flyer Manuale - CON WATERMARK PAGINE SINGOLEDokument6 SeitenFlyer Manuale - CON WATERMARK PAGINE SINGOLEjscmtNoch keine Bewertungen
- Gowtham Kumar Chitturi - HRMS Technical - 6 YrsDokument4 SeitenGowtham Kumar Chitturi - HRMS Technical - 6 YrsAnuNoch keine Bewertungen
- Idmt Curve CalulationDokument5 SeitenIdmt Curve CalulationHimesh NairNoch keine Bewertungen
- Consultancy Services For The Feasibility Study of A Second Runway at SSR International AirportDokument6 SeitenConsultancy Services For The Feasibility Study of A Second Runway at SSR International AirportNitish RamdaworNoch keine Bewertungen
- Unit List MUZAFFARPUR - Feb 18 PDFDokument28 SeitenUnit List MUZAFFARPUR - Feb 18 PDFPawan Kumar100% (1)
- Resources and Courses: Moocs (Massive Open Online Courses)Dokument8 SeitenResources and Courses: Moocs (Massive Open Online Courses)Jump SkillNoch keine Bewertungen
- Moparm Action - December 2014 USADokument100 SeitenMoparm Action - December 2014 USAenricoioNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 01 RFI Technical Form BiodataDokument8 Seiten01 RFI Technical Form BiodataRafiq RizkiNoch keine Bewertungen
- Seminar Report of Automatic Street Light: Presented byDokument14 SeitenSeminar Report of Automatic Street Light: Presented byTeri Maa Ki100% (2)
- Province of Camarines Sur vs. CADokument8 SeitenProvince of Camarines Sur vs. CACrisDBNoch keine Bewertungen
- Unit 10-Maintain Knowledge of Improvements To Influence Health and Safety Practice ARDokument9 SeitenUnit 10-Maintain Knowledge of Improvements To Influence Health and Safety Practice ARAshraf EL WardajiNoch keine Bewertungen
- S 101-01 - PDF - User Interface - Computer MonitorDokument130 SeitenS 101-01 - PDF - User Interface - Computer Monitormborghesi1Noch keine Bewertungen
- Irrig in AfricaDokument64 SeitenIrrig in Africaer viNoch keine Bewertungen
- Auto Report LogDokument3 SeitenAuto Report LogDaniel LermaNoch keine Bewertungen
- Effective Communication LeaderDokument4 SeitenEffective Communication LeaderAnggun PraditaNoch keine Bewertungen
- Verma Toys Leona Bebe PDFDokument28 SeitenVerma Toys Leona Bebe PDFSILVIA ROMERO100% (3)
- SKF LGMT-2 Data SheetDokument2 SeitenSKF LGMT-2 Data SheetRahul SharmaNoch keine Bewertungen
- Risk and Uncertainty in Estimating and TenderingDokument16 SeitenRisk and Uncertainty in Estimating and TenderingHaneefa ChNoch keine Bewertungen
- QP 4Dokument4 SeitenQP 4Yusra RaoufNoch keine Bewertungen
- Pyro ShieldDokument6 SeitenPyro Shieldmunim87Noch keine Bewertungen
- Pharmaceutical Microbiology NewsletterDokument12 SeitenPharmaceutical Microbiology NewsletterTim SandleNoch keine Bewertungen
- CW February 2013Dokument60 SeitenCW February 2013Clint FosterNoch keine Bewertungen
- Electric Arc Furnace STEEL MAKINGDokument28 SeitenElectric Arc Furnace STEEL MAKINGAMMASI A SHARAN100% (3)
- Self-Instructional Manual (SIM) For Self-Directed Learning (SDL)Dokument28 SeitenSelf-Instructional Manual (SIM) For Self-Directed Learning (SDL)Monique Dianne Dela VegaNoch keine Bewertungen
- Dreamfoil Creations & Nemeth DesignsDokument22 SeitenDreamfoil Creations & Nemeth DesignsManoel ValentimNoch keine Bewertungen
- Man Machine Interface SafetyDokument9 SeitenMan Machine Interface SafetyVidyesh Viswanathan NairNoch keine Bewertungen
- Singapore Electricity MarketDokument25 SeitenSingapore Electricity MarketTonia GlennNoch keine Bewertungen
- Company Law Handout 3Dokument10 SeitenCompany Law Handout 3nicoleclleeNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)