Das könnte Ihnen auch gefallen
- GYNE UltrasoundgyneDokument11 SeitenGYNE UltrasoundgyneMara AbantoNoch keine Bewertungen
- Diaphragmatic Eventration Presenting As A Recurrent Diaphragmatic HerniaDokument4 SeitenDiaphragmatic Eventration Presenting As A Recurrent Diaphragmatic HerniaHesti hasanNoch keine Bewertungen
- Anterior Open-Bite - A Cephalometric Analysis and Suggested Treatment ProceduresDokument9 SeitenAnterior Open-Bite - A Cephalometric Analysis and Suggested Treatment ProceduresRenan MotaNoch keine Bewertungen
- 01 - PediatricsDokument74 Seiten01 - Pediatricscore radiologyNoch keine Bewertungen
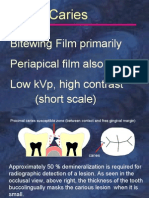
- Caries Perio LocalizationDokument141 SeitenCaries Perio LocalizationAmany SulimanNoch keine Bewertungen
- Surgical Management of Right Colon DiverticulitisDokument4 SeitenSurgical Management of Right Colon DiverticulitisDimas De Conti GramzNoch keine Bewertungen
- Phlebography in Superior Vena Caval: Obstruction'Dokument5 SeitenPhlebography in Superior Vena Caval: Obstruction'Diva PrayogaNoch keine Bewertungen
- Myelography in ChildrenDokument16 SeitenMyelography in ChildrenFinna Tryasti Fidianti1BNoch keine Bewertungen
- Carli Claudo MarDokument4 SeitenCarli Claudo MarMedardo ApoloNoch keine Bewertungen
- Past History. - The Physical Examination - Physical: Harry J - Cohen, and Paul J - Caivieron, New York, N. YDokument4 SeitenPast History. - The Physical Examination - Physical: Harry J - Cohen, and Paul J - Caivieron, New York, N. YReza Alfitra MutiaraNoch keine Bewertungen
- Hernia InguinalDokument18 SeitenHernia InguinalisabellaNoch keine Bewertungen
- Cerebrospinal Fluid Leaks: Michael E. Decherd, MD Byron J. Bailey, MD May 26, 1999Dokument6 SeitenCerebrospinal Fluid Leaks: Michael E. Decherd, MD Byron J. Bailey, MD May 26, 1999Lina PratiwiNoch keine Bewertungen
- Chest RadiographyDokument19 SeitenChest RadiographyClaraMonet PalomoNoch keine Bewertungen
- RectumDokument129 SeitenRectumRadhika SethuNoch keine Bewertungen
- Soleimani 2007Dokument9 SeitenSoleimani 2007ceciliaNoch keine Bewertungen
- Gastrointestinal SurgeryDokument78 SeitenGastrointestinal Surgeryjjmail100% (1)
- Pelvic Floor Ultrasound - A Review - 220211 - 100603Dokument24 SeitenPelvic Floor Ultrasound - A Review - 220211 - 100603Mariana Larroulet SantanderNoch keine Bewertungen
- HovariDokument4 SeitenHovarismoothstuff87Noch keine Bewertungen
- Acute Abdominal Pain From Upper Urinary Tract Lesions: OrdinaryDokument4 SeitenAcute Abdominal Pain From Upper Urinary Tract Lesions: OrdinaryivanNoch keine Bewertungen
- Retroperitoneal Appendicitis: A Surgical DilemmaDokument2 SeitenRetroperitoneal Appendicitis: A Surgical DilemmaputraNoch keine Bewertungen
- Long-Term Results of Lateral Internal Sphincterotomy For Chronic Anal Fissure With Particular Reference To Incidence of Fecal IncontinenceDokument5 SeitenLong-Term Results of Lateral Internal Sphincterotomy For Chronic Anal Fissure With Particular Reference To Incidence of Fecal IncontinenceMetin AzaNoch keine Bewertungen
- Management of T.B.M. Hydrocephalus Role of Shunt Surgery - 55 58Dokument4 SeitenManagement of T.B.M. Hydrocephalus Role of Shunt Surgery - 55 58Kushal BhatiaNoch keine Bewertungen
- Sequelae of Traumatic and Pathologic Changes: The Orthodontist's ViewpointDokument9 SeitenSequelae of Traumatic and Pathologic Changes: The Orthodontist's ViewpointShreyaNoch keine Bewertungen
- Lazarus SyndromeDokument4 SeitenLazarus SyndromeEugeni meldaNoch keine Bewertungen
- PositioningDokument97 SeitenPositioningzixdiddy100% (1)
- Nbme Step 1 AnatomyDokument23 SeitenNbme Step 1 AnatomyMohsin Farooq100% (12)
- Duodenal Atresia Neewborn: in TheDokument18 SeitenDuodenal Atresia Neewborn: in TheIndah Permata SariNoch keine Bewertungen
- المضارع البسيط موقعDokument6 Seitenالمضارع البسيط موقعabdulfatahalhemeryNoch keine Bewertungen
- Laparoscopic Hernia Repair in Neonates, Infants and ChildrenDokument9 SeitenLaparoscopic Hernia Repair in Neonates, Infants and ChildrenErick OematanNoch keine Bewertungen
- Ruiz, P. - SGD and NCP On Imperforate AnusDokument8 SeitenRuiz, P. - SGD and NCP On Imperforate AnusPatricia Dianne RuizNoch keine Bewertungen
- Cardiovascular MCQsDokument23 SeitenCardiovascular MCQssb medexNoch keine Bewertungen
- Ortho SBA OrthobulletDokument168 SeitenOrtho SBA Orthobulletayunisalleh88% (8)
- R Aofoct: HypertrophyDokument4 SeitenR Aofoct: HypertrophyGagandeep SinghNoch keine Bewertungen
- Referensi (12), 14 - Anorectal MalformationsDokument9 SeitenReferensi (12), 14 - Anorectal MalformationsAsbar Fatur MuhNoch keine Bewertungen
- How To Read An Abdominal XrayDokument38 SeitenHow To Read An Abdominal Xraytwentyjazzfunkgreats3055100% (1)
- Imperforate Hymen Complicated by Obstructive Acute Renal FailureDokument3 SeitenImperforate Hymen Complicated by Obstructive Acute Renal FailureQonny WelendriNoch keine Bewertungen
- Blunt Pelviperineal InjuriesDokument4 SeitenBlunt Pelviperineal InjuriesAhmadNassrNoch keine Bewertungen
- Umbilical HerniapdfDokument16 SeitenUmbilical HerniapdfAimie Farhanah Binti ZakariaNoch keine Bewertungen
- The 3rd Edition: Prevention & Management: Complications of Laparoscopic Inguinal Hernia RepairDokument5 SeitenThe 3rd Edition: Prevention & Management: Complications of Laparoscopic Inguinal Hernia RepairVishnu KumarNoch keine Bewertungen
- 08 Trans Perineal UltrasoundDokument4 Seiten08 Trans Perineal UltrasoundArif BudimanNoch keine Bewertungen
- Slide, Tracheal BronchusDokument4 SeitenSlide, Tracheal Bronchusemmanuel le bretNoch keine Bewertungen
- 199 FullDokument8 Seiten199 Fullryanv0621Noch keine Bewertungen
- Abdomen: International Abstracts of Pediatric Surgery 593Dokument1 SeiteAbdomen: International Abstracts of Pediatric Surgery 593Yohanes WilliamNoch keine Bewertungen
- US Hip TechniqueDokument8 SeitenUS Hip TechniqueAdam JonesNoch keine Bewertungen
- Incarceratedpediatric Hernias: Sophia A. Abdulhai,, Ian C. Glenn,, Todd A. PonskyDokument17 SeitenIncarceratedpediatric Hernias: Sophia A. Abdulhai,, Ian C. Glenn,, Todd A. PonskyPhytoplankton DiatomsNoch keine Bewertungen
- Surgical Techniques: Plication of The DiaphragmDokument14 SeitenSurgical Techniques: Plication of The DiaphragmFranciscoJ.ReynaSepúlvedaNoch keine Bewertungen
- ATLS Practice Test 2 Answers & ExplanationsDokument8 SeitenATLS Practice Test 2 Answers & Explanationsemad mohamedNoch keine Bewertungen
- Gomella Sec03 p0167 0300Dokument134 SeitenGomella Sec03 p0167 0300Gabriela GheorgheNoch keine Bewertungen
- Handbook HerniaDokument8 SeitenHandbook HerniaDian PuspaNoch keine Bewertungen
- Presentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONDokument23 SeitenPresentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONMubarak M AlkaliNoch keine Bewertungen
- Unas November 2019Dokument21 SeitenUnas November 2019Muhammad FaisalNoch keine Bewertungen
- Síndrome Adrenogenital e Alterações Anatômicas PDFDokument10 SeitenSíndrome Adrenogenital e Alterações Anatômicas PDFFred SilvaNoch keine Bewertungen
- Fibrous Mastopathy in Insulin Dependent Diabetics: Clinical RadiologyDokument3 SeitenFibrous Mastopathy in Insulin Dependent Diabetics: Clinical RadiologyHarshoi KrishannaNoch keine Bewertungen
- Hospital, Although: Treatment StrabismusDokument3 SeitenHospital, Although: Treatment StrabismusPopescuNoch keine Bewertungen
- Lazard 1996Dokument2 SeitenLazard 1996Timpswalo EmatsuloNoch keine Bewertungen
- Estenos PiloricaDokument7 SeitenEstenos Piloricadayanita1221Noch keine Bewertungen
- 01 Ajpcr 46717Dokument3 Seiten01 Ajpcr 46717DipteshPatilNoch keine Bewertungen
- Laparoscopic Appendectomy: Samir DelibegovićDokument7 SeitenLaparoscopic Appendectomy: Samir DelibegovićKamran AfzalNoch keine Bewertungen
- Anatomy BMJOnExamination 2016Dokument89 SeitenAnatomy BMJOnExamination 2016jmoNoch keine Bewertungen
- "A Hospital": Operations RoomDokument7 Seiten"A Hospital": Operations RoomApple IdeaNoch keine Bewertungen
- A Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleDokument5 SeitenA Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleApple IdeaNoch keine Bewertungen
- Tanggal Nama Usia DiagnosisDokument6 SeitenTanggal Nama Usia DiagnosisApple IdeaNoch keine Bewertungen
- Sprai Homemade "SUN'S COLLECTION" Motif KALTIMDokument1 SeiteSprai Homemade "SUN'S COLLECTION" Motif KALTIMApple IdeaNoch keine Bewertungen
- Dermatomycological Profile of Patients in A Tertiary Care Hospital of Western MaharashtraDokument2 SeitenDermatomycological Profile of Patients in A Tertiary Care Hospital of Western MaharashtraApple IdeaNoch keine Bewertungen
- By Product "Simpang Raya Baby" Jln. Hamm Rifaddin No.2 Samarinda Seberang HP. 0812 5732 6335Dokument1 SeiteBy Product "Simpang Raya Baby" Jln. Hamm Rifaddin No.2 Samarinda Seberang HP. 0812 5732 6335Apple IdeaNoch keine Bewertungen
- Gastric VolvulusDokument7 SeitenGastric Volvuluswilson koresNoch keine Bewertungen
- Gastro-Esophageal Reflux Disease ( GERD)Dokument31 SeitenGastro-Esophageal Reflux Disease ( GERD)Malueth AnguiNoch keine Bewertungen
- Chirurgie 1 Teste VozianDokument47 SeitenChirurgie 1 Teste Voziangm hashNoch keine Bewertungen
- Clinical Cases and Osces in SurgeryDokument278 SeitenClinical Cases and Osces in SurgeryTristan Greene100% (5)
- Umbilical Hernia RepairDokument11 SeitenUmbilical Hernia RepairMantu DasNoch keine Bewertungen
- Medical Surgical Nursing Nclex questionsGI1Dokument11 SeitenMedical Surgical Nursing Nclex questionsGI1dee_day_8100% (2)
- Small Bowel Obstruction - Clinical Diagnosis and TreatmentDokument11 SeitenSmall Bowel Obstruction - Clinical Diagnosis and TreatmentVigariooNoch keine Bewertungen
- CWU 1 SurgeryDokument23 SeitenCWU 1 SurgeryAmelia AkmarNoch keine Bewertungen
- Front of Thigh NotesDokument8 SeitenFront of Thigh NotesMeowNoch keine Bewertungen
- Duhs Surgery Past Papers 2011-2017 DRDokument164 SeitenDuhs Surgery Past Papers 2011-2017 DRRaffles HolmesNoch keine Bewertungen
- Incisional HerniaDokument14 SeitenIncisional Herniaelene nikoleishviliNoch keine Bewertungen
- ABDOMEN124Dokument25 SeitenABDOMEN124Ashraf Alamin AhmedNoch keine Bewertungen
- 194 Surgical Cases PDFDokument160 Seiten194 Surgical Cases PDFkint100% (4)
- Surgery Revalida Review PDFDokument11 SeitenSurgery Revalida Review PDFMara Medina - BorleoNoch keine Bewertungen
- Abdominal Walls - HB 2Dokument92 SeitenAbdominal Walls - HB 2akosuaaniiwaa09Noch keine Bewertungen
- New York Medicaid APG CrosswalkDokument6.734 SeitenNew York Medicaid APG CrosswalksdpetesrhsNoch keine Bewertungen
- Review of Internal HerniasDokument15 SeitenReview of Internal HerniassavingtaviaNoch keine Bewertungen
- Initial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryDokument6 SeitenInitial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryilhamNoch keine Bewertungen
- Abdominal HerniaDokument4 SeitenAbdominal HerniaDr. mohammed AbdulhameedNoch keine Bewertungen
- Inguinoscrotal Swelling in PediatricsDokument84 SeitenInguinoscrotal Swelling in Pediatricshayssam rashwan90% (10)
- Dinding Abdomen PSIKDokument79 SeitenDinding Abdomen PSIKSondang DamanikNoch keine Bewertungen
- Clinical Examination NOTESDokument11 SeitenClinical Examination NOTESDanielDzinotyiweiD-cubedNoch keine Bewertungen
- General Surgery-Master and DiplomaDokument3 SeitenGeneral Surgery-Master and DiplomaMohamed ElfekyNoch keine Bewertungen
- Minimally Invasive Surgery: Amar Shah and Anirudh ShahDokument5 SeitenMinimally Invasive Surgery: Amar Shah and Anirudh ShahKadelsy BristolNoch keine Bewertungen
- Git Surgery 4 Year 2022 NebrasDokument9 SeitenGit Surgery 4 Year 2022 NebrasHazemAbu-BakrNoch keine Bewertungen
- Assessing Female Genitourinary SystemDokument6 SeitenAssessing Female Genitourinary SystemJo Marchianne PigarNoch keine Bewertungen
- Hernia: Done by D1 GroupDokument47 SeitenHernia: Done by D1 Groupanindyadputri100% (1)
- IPHS Guidelines District HospitalDokument120 SeitenIPHS Guidelines District HospitalMohd Salahuddin100% (1)
- Case Report Amayand, S HerniaDokument13 SeitenCase Report Amayand, S HerniaJavaidIqbalNoch keine Bewertungen
- Abdominal Wall, Omentum, Mesentery and RetroperitoneumDokument8 SeitenAbdominal Wall, Omentum, Mesentery and RetroperitoneumRae Marie AquinoNoch keine Bewertungen