Das könnte Ihnen auch gefallen
- 12 Houses ExplainedDokument3 Seiten12 Houses ExplainedKoshi EnterprisesNoch keine Bewertungen
- Mixing Studies 1pp 08-13-15.pptx 0 PDFDokument49 SeitenMixing Studies 1pp 08-13-15.pptx 0 PDFKholifah LintangNoch keine Bewertungen
- Neurovascular Holding PointsDokument8 SeitenNeurovascular Holding PointsAlexandru Baciu100% (1)
- Scientific Writing VerbsDokument3 SeitenScientific Writing VerbsNejdetEXn100% (1)
- O Level Physics QuestionsDokument9 SeitenO Level Physics QuestionsMichael Leung67% (3)
- Topic 3 BatteryDokument40 SeitenTopic 3 BatterynisaNoch keine Bewertungen
- Spouses Benatiro V CuyosDokument1 SeiteSpouses Benatiro V CuyosAleli BucuNoch keine Bewertungen
- BANDAGINGDokument6 SeitenBANDAGINGSweet BenitezNoch keine Bewertungen
- Philippine Urological Association, Inc.: Executive Committee and Board Members 1997Dokument12 SeitenPhilippine Urological Association, Inc.: Executive Committee and Board Members 1997mits98Noch keine Bewertungen
- Utmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherDokument210 SeitenUtmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherTrish HồNoch keine Bewertungen
- Types of Drills PDFDokument8 SeitenTypes of Drills PDFSummer nightsNoch keine Bewertungen
- Epigenetics (Nilofer Saba Azad, M.D.)Dokument40 SeitenEpigenetics (Nilofer Saba Azad, M.D.)National Press Foundation100% (1)
- Mendezona vs. OzamizDokument2 SeitenMendezona vs. OzamizAlexis Von TeNoch keine Bewertungen
- Anticoagulant DOACDokument39 SeitenAnticoagulant DOACSukmawatiNoch keine Bewertungen
- Drug Monograph ExampleDokument6 SeitenDrug Monograph ExampleAaltiyaNoch keine Bewertungen
- VTE Form - Surgical & Medical PatientsDokument2 SeitenVTE Form - Surgical & Medical PatientsNatasha BhasinNoch keine Bewertungen
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dokument26 SeitenXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNoch keine Bewertungen
- Arni PPT 2 PDFDokument19 SeitenArni PPT 2 PDFKumarsai Durusoju100% (1)
- New Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011Dokument55 SeitenNew Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011andresrgomezNoch keine Bewertungen
- Blockade R A SDokument20 SeitenBlockade R A SAlaa KhazalehNoch keine Bewertungen
- The Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasDokument29 SeitenThe Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasHerry HendrayadiNoch keine Bewertungen
- NOACs DOACs Coagulation Tests 2018nov16Dokument5 SeitenNOACs DOACs Coagulation Tests 2018nov16Agam AsikNoch keine Bewertungen
- Atorvastatin Statin in CVD ManagementDokument37 SeitenAtorvastatin Statin in CVD ManagementSriNoch keine Bewertungen
- Statins in CVD Management: Is Just Lipid Lowering Enough?Dokument37 SeitenStatins in CVD Management: Is Just Lipid Lowering Enough?SriNoch keine Bewertungen
- (FINAL) Prof Tschope - Challenges I HF Management How To Address Unmet NeedsDokument38 Seiten(FINAL) Prof Tschope - Challenges I HF Management How To Address Unmet NeedsTicksNoch keine Bewertungen
- IsarreactDokument4 SeitenIsarreactLeow Khang LengNoch keine Bewertungen
- Non-Steroidal Anti-Inflammatory Drugs (Nsaids 3)Dokument35 SeitenNon-Steroidal Anti-Inflammatory Drugs (Nsaids 3)Sophia LiuNoch keine Bewertungen
- Van de Werf Re-AlignDokument9 SeitenVan de Werf Re-AlignClayton JensenNoch keine Bewertungen
- Angiotensin Receptor Neprilysin Inhibition (ARNI) Following Acute Myocardial Infarction: Primary Results of The PARADISE-MI TrialDokument26 SeitenAngiotensin Receptor Neprilysin Inhibition (ARNI) Following Acute Myocardial Infarction: Primary Results of The PARADISE-MI TrialsumaNoch keine Bewertungen
- Cytotoxic Chemotherapy Produces Limited Benefit in Stage IV NSCLCDokument10 SeitenCytotoxic Chemotherapy Produces Limited Benefit in Stage IV NSCLCAnich DevaNoch keine Bewertungen
- CCU 2017 AntiplateletDokument22 SeitenCCU 2017 AntiplateletDhinie NovianiNoch keine Bewertungen
- The Role of Antithrombin III in Neonatal Sepsis - Novie AmeliaDokument26 SeitenThe Role of Antithrombin III in Neonatal Sepsis - Novie AmeliaBayu KurniawanNoch keine Bewertungen
- Non - Invasive Ventilation - Setting Up A ServiceDokument30 SeitenNon - Invasive Ventilation - Setting Up A ServiceArtem 521Noch keine Bewertungen
- Afib For JCU 2Dokument33 SeitenAfib For JCU 2Sofia KusumadewiNoch keine Bewertungen
- VTE Form - Surgical & Medical PatientsDokument2 SeitenVTE Form - Surgical & Medical PatientsNatasha BhasinNoch keine Bewertungen
- Pro Common Pediatric EmergenciesDokument36 SeitenPro Common Pediatric EmergenciesyasuyahyajpnNoch keine Bewertungen
- Noxarin Brosur-MinDokument4 SeitenNoxarin Brosur-MinAndy RahadianNoch keine Bewertungen
- New in Heart Failure - VericiguatDokument38 SeitenNew in Heart Failure - Vericiguatapi-536775958Noch keine Bewertungen
- Grand RoundsDokument55 SeitenGrand Roundsapi-716714980Noch keine Bewertungen
- IvabradineDokument30 SeitenIvabradinepashaNoch keine Bewertungen
- Slides Outcomes of Sglt2i in Diabetic Kidney Disease Is It All DiabetesDokument29 SeitenSlides Outcomes of Sglt2i in Diabetic Kidney Disease Is It All DiabetesVaibhav DafaleNoch keine Bewertungen
- PCPDokument6 SeitenPCPBob BobNoch keine Bewertungen
- Anticoagulant Up123Dokument15 SeitenAnticoagulant Up123ahmed khaledNoch keine Bewertungen
- Venous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDDokument23 SeitenVenous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDعزالدين الطيارNoch keine Bewertungen
- Dapa Brief Data (14271)Dokument24 SeitenDapa Brief Data (14271)Adel SALLAM100% (1)
- PE Masalah Di Indonesia ISSHPDokument53 SeitenPE Masalah Di Indonesia ISSHPDillyani PurnamaNoch keine Bewertungen
- Medication Worksheet: Citrus College Associate Degree NursingDokument5 SeitenMedication Worksheet: Citrus College Associate Degree NursingRhonnie De GuzmanNoch keine Bewertungen
- Ate GlendaDokument3 SeitenAte GlendaRomel Ricafort John DavidNoch keine Bewertungen
- The REGULATE-PCI Randomized Clinical TrialDokument26 SeitenThe REGULATE-PCI Randomized Clinical TrialstacayNoch keine Bewertungen
- Activase (Alteplase) in Acute Ischemic Stroke: Frequently Asked Questions AboutDokument16 SeitenActivase (Alteplase) in Acute Ischemic Stroke: Frequently Asked Questions AboutHappiness ProjectNoch keine Bewertungen
- Response Assessment in Neuro-Oncology (RANO)Dokument31 SeitenResponse Assessment in Neuro-Oncology (RANO)Rini AndrianiNoch keine Bewertungen
- Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)Dokument26 SeitenNonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)ROHITNoch keine Bewertungen
- Curriculum Vitae: Lulus Handayani, MDDokument31 SeitenCurriculum Vitae: Lulus Handayani, MDpisangphoeNoch keine Bewertungen
- Secondary HLH Case Report: Highlighting Clinical ChallengesDokument11 SeitenSecondary HLH Case Report: Highlighting Clinical ChallengesDr. Surya Abadi KristyoadiNoch keine Bewertungen
- Ob Rev2004Dokument7 SeitenOb Rev2004raceforthechase07Noch keine Bewertungen
- Non ST Elevation Acs Optimizing Anti Thrombotic TherapyDokument20 SeitenNon ST Elevation Acs Optimizing Anti Thrombotic TherapydcicareNoch keine Bewertungen
- Paradise TrialDokument26 SeitenParadise TrialMiguel Martinez DuranNoch keine Bewertungen
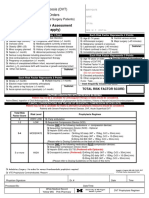
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDokument2 SeitenThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNoch keine Bewertungen
- Estimasi Jumlah Perdarahan Dan Syok Yudianto 2017Dokument9 SeitenEstimasi Jumlah Perdarahan Dan Syok Yudianto 2017Mocco PpumumNoch keine Bewertungen
- AFib WarfarinVsNOACsDokument2 SeitenAFib WarfarinVsNOACsalpha wolfNoch keine Bewertungen
- GAGAN Male2 Years 42055Dokument1 SeiteGAGAN Male2 Years 42055C MNoch keine Bewertungen
- Daftar Follow Up Pasien Covid-19 Atensi: Detasemen Kesehatan Wilayah 12.04.02 Rumah Sakit TK Iv 12.07.03Dokument4 SeitenDaftar Follow Up Pasien Covid-19 Atensi: Detasemen Kesehatan Wilayah 12.04.02 Rumah Sakit TK Iv 12.07.03rstpalangkaraya rstpalangkarayaNoch keine Bewertungen
- PDF Nursing Care PlanDokument16 SeitenPDF Nursing Care PlanMichael MabiniNoch keine Bewertungen
- Rivaroxaban PresentationDokument13 SeitenRivaroxaban PresentationReem El-HusseinyNoch keine Bewertungen
- RENAAL Overview: Brenner BM, Et Al. N Engl J Med. 2001 345 (12) :861-869Dokument7 SeitenRENAAL Overview: Brenner BM, Et Al. N Engl J Med. 2001 345 (12) :861-869ekadtorNoch keine Bewertungen
- Recurrent TonsilitisDokument16 SeitenRecurrent TonsilitisAyen FornollesNoch keine Bewertungen
- Update On The Medical Management of Acute Coronary SyndromeDokument47 SeitenUpdate On The Medical Management of Acute Coronary SyndromeykaramangNoch keine Bewertungen
- CCO IBD Key Issues Downloadable 4Dokument22 SeitenCCO IBD Key Issues Downloadable 4160835Noch keine Bewertungen
- Lab Results: Thrivikraman Subramanian Irene Rummel, PA-CDokument3 SeitenLab Results: Thrivikraman Subramanian Irene Rummel, PA-CJackeline PaezNoch keine Bewertungen
- Petunjuk Kesehatan Dalam Al Quran Dan Sunnah 6 April 2010Dokument53 SeitenPetunjuk Kesehatan Dalam Al Quran Dan Sunnah 6 April 2010Emdan SengadjiNoch keine Bewertungen
- Petunjuk Kesehatan Dalam Al Quran Dan Sunnah 6 April 2010Dokument53 SeitenPetunjuk Kesehatan Dalam Al Quran Dan Sunnah 6 April 2010Emdan SengadjiNoch keine Bewertungen
- ALO Optimal Anticoagulant FinalDokument19 SeitenALO Optimal Anticoagulant FinalEmdan SengadjiNoch keine Bewertungen
- Workshop 3rdbkcu Christine 2Dokument17 SeitenWorkshop 3rdbkcu Christine 2Emdan SengadjiNoch keine Bewertungen
- ALO Optimal Anticoagulant FinalDokument19 SeitenALO Optimal Anticoagulant FinalEmdan SengadjiNoch keine Bewertungen
- Migraine Current Treatment and Emerging Therapies PDFDokument11 SeitenMigraine Current Treatment and Emerging Therapies PDFEmdan SengadjiNoch keine Bewertungen
- Refleks VagusDokument45 SeitenRefleks VagusEmdan SengadjiNoch keine Bewertungen
- Inne Pratiwi F.G2A008097.KTIDokument83 SeitenInne Pratiwi F.G2A008097.KTIEmdan SengadjiNoch keine Bewertungen
- DRDokument18 SeitenDREmdan SengadjiNoch keine Bewertungen
- Refleks VagusDokument45 SeitenRefleks VagusEmdan SengadjiNoch keine Bewertungen
- Khutbah Jum'at Save Al Quds Save PalestinaDokument10 SeitenKhutbah Jum'at Save Al Quds Save PalestinaEmdan SengadjiNoch keine Bewertungen
- Refleks VagusDokument45 SeitenRefleks VagusEmdan SengadjiNoch keine Bewertungen
- Dr. Saifur Anticoagulant in ACS PDFDokument61 SeitenDr. Saifur Anticoagulant in ACS PDFEmdan SengadjiNoch keine Bewertungen
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDokument18 SeitenGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiNoch keine Bewertungen
- Inne Pratiwi F.G2A008097.KTIDokument83 SeitenInne Pratiwi F.G2A008097.KTIEmdan SengadjiNoch keine Bewertungen
- DRDokument18 SeitenDREmdan SengadjiNoch keine Bewertungen
- DRDokument18 SeitenDREmdan SengadjiNoch keine Bewertungen
- Cold InjuryDokument9 SeitenCold InjuryFina Ahmad FitrianaNoch keine Bewertungen
- DR Cholid - Non Pharmacologic Management in Heart Failure PDFDokument37 SeitenDR Cholid - Non Pharmacologic Management in Heart Failure PDFEmdan SengadjiNoch keine Bewertungen
- Migraine Current Treatment and Emerging Therapies PDFDokument11 SeitenMigraine Current Treatment and Emerging Therapies PDFEmdan SengadjiNoch keine Bewertungen
- Dr. Saifur Anticoagulant in ACS PDFDokument61 SeitenDr. Saifur Anticoagulant in ACS PDFEmdan SengadjiNoch keine Bewertungen
- DR Cholid - Non Pharmacologic Management in Heart Failure PDFDokument37 SeitenDR Cholid - Non Pharmacologic Management in Heart Failure PDFEmdan SengadjiNoch keine Bewertungen
- Khutbah Jum'at Birrul Walidain PDFDokument10 SeitenKhutbah Jum'at Birrul Walidain PDFEmdan Sengadji0% (1)
- DRDokument18 SeitenDREmdan SengadjiNoch keine Bewertungen
- Khotbah JumadDokument11 SeitenKhotbah JumadEmdan SengadjiNoch keine Bewertungen
- Khutbah Jum'at Nikmat Adzab KuburDokument10 SeitenKhutbah Jum'at Nikmat Adzab KuburEmdan SengadjiNoch keine Bewertungen
- Electrolyte Imbalance 15102017Dokument34 SeitenElectrolyte Imbalance 15102017Emdan SengadjiNoch keine Bewertungen
- Ed enDokument358 SeitenEd enLuqman HakimNoch keine Bewertungen
- Clinical Approach To AFDokument32 SeitenClinical Approach To AFEmdan SengadjiNoch keine Bewertungen
- Dwnload Full Social Psychology 4th Edition Gilovich Test Bank PDFDokument35 SeitenDwnload Full Social Psychology 4th Edition Gilovich Test Bank PDFalilonghidotardlyq71i7f100% (8)
- Synopss Orignal of Ambuja CementDokument25 SeitenSynopss Orignal of Ambuja CementLovely Garima JainNoch keine Bewertungen
- Chapter 1 To 3. Methods of ResearchDokument18 SeitenChapter 1 To 3. Methods of ResearchMaryAnnLasquiteNoch keine Bewertungen
- Education Is The Foundation For Women Empowerment in IndiaDokument111 SeitenEducation Is The Foundation For Women Empowerment in IndiaAmit Kumar ChoudharyNoch keine Bewertungen
- Prior-To-Class Quiz 10 - Statistics For Business-T123PWB-1Dokument6 SeitenPrior-To-Class Quiz 10 - Statistics For Business-T123PWB-1Minhh HằnggNoch keine Bewertungen
- Egg Osmosis PosterDokument2 SeitenEgg Osmosis Posterapi-496477356Noch keine Bewertungen
- 19 March 2018 CcmaDokument4 Seiten19 March 2018 Ccmabronnaf80Noch keine Bewertungen
- Disseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractDokument3 SeitenDisseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractAmelia Fitria DewiNoch keine Bewertungen
- Hemzo M. Marketing Luxury Services. Concepts, Strategy and Practice 2023Dokument219 SeitenHemzo M. Marketing Luxury Services. Concepts, Strategy and Practice 2023ichigosonix66Noch keine Bewertungen
- The Tamil Nadu Commercial Taxes ServiceDokument9 SeitenThe Tamil Nadu Commercial Taxes ServiceKumar AvelNoch keine Bewertungen
- Reflection Chapter 13 and 14Dokument2 SeitenReflection Chapter 13 and 14Vanessa Zevallos HernandezNoch keine Bewertungen
- Artificial Neural NetworkDokument16 SeitenArtificial Neural NetworkSahil ChopraNoch keine Bewertungen
- Legal Insights Issue 4 2018Dokument24 SeitenLegal Insights Issue 4 2018Weicong TanNoch keine Bewertungen
- Alternative Forms of BusOrgDokument16 SeitenAlternative Forms of BusOrgnatalie clyde matesNoch keine Bewertungen
- DLP IN LitDokument9 SeitenDLP IN LitLotis VallanteNoch keine Bewertungen
- Simplified Analysis of 'Out, Out' - Robert FrostDokument3 SeitenSimplified Analysis of 'Out, Out' - Robert FrostSANDREA RUTHNoch keine Bewertungen
- Kerkythea Material Editor Guide 01Dokument36 SeitenKerkythea Material Editor Guide 01sapomasterNoch keine Bewertungen
- WaveDokument5 SeitenWaveArijitSherlockMudiNoch keine Bewertungen
- AP Macroeconomics: About The Advanced Placement Program (AP)Dokument2 SeitenAP Macroeconomics: About The Advanced Placement Program (AP)Adam NowickiNoch keine Bewertungen
- Thesis Project Management SoftwareDokument7 SeitenThesis Project Management Softwarehollyschulzgilbert100% (2)
- Question Bank of Financial Management - 2markDokument16 SeitenQuestion Bank of Financial Management - 2marklakkuMSNoch keine Bewertungen