Das könnte Ihnen auch gefallen
- Understanding Multinodular Non-Toxic GoiterDokument58 SeitenUnderstanding Multinodular Non-Toxic GoiterSeff CausapinNoch keine Bewertungen
- Dem Tickler NotesDokument1 SeiteDem Tickler NotesSeff CausapinNoch keine Bewertungen
- Anterior Pituitary Tumor SyndromesDokument10 SeitenAnterior Pituitary Tumor SyndromesSeff CausapinNoch keine Bewertungen
- Urinary Tract Obstruction (UTO): Causes, Symptoms and DiagnosisDokument2 SeitenUrinary Tract Obstruction (UTO): Causes, Symptoms and DiagnosisSeff CausapinNoch keine Bewertungen
- Hemostasissurgicalbleedingandtransfusion 130707035616 Phpapp02Dokument42 SeitenHemostasissurgicalbleedingandtransfusion 130707035616 Phpapp02Seff CausapinNoch keine Bewertungen
- Anterior Pituitary Tumor SyndromesDokument10 SeitenAnterior Pituitary Tumor SyndromesSeff CausapinNoch keine Bewertungen
- Disorders of The Female Reproductive System PDFDokument4 SeitenDisorders of The Female Reproductive System PDFSeff CausapinNoch keine Bewertungen
- 3 180824051636Dokument45 Seiten3 180824051636Seff CausapinNoch keine Bewertungen
- Altitude IllnessDokument4 SeitenAltitude IllnessSeff CausapinNoch keine Bewertungen
- Disorders of The Female Reproductive System PDFDokument4 SeitenDisorders of The Female Reproductive System PDFSeff CausapinNoch keine Bewertungen
- Glomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesDokument6 SeitenGlomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesSeff CausapinNoch keine Bewertungen
- Lumbar TapDokument4 SeitenLumbar TapSeff CausapinNoch keine Bewertungen
- Medicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Dokument3 SeitenMedicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Seff CausapinNoch keine Bewertungen
- Approach To Patient With Endocrine DisordersDokument2 SeitenApproach To Patient With Endocrine DisordersSeff CausapinNoch keine Bewertungen
- Complete Guide To Physical ExamDokument19 SeitenComplete Guide To Physical ExamSeff Causapin100% (2)
- Approach To The PX With CancerDokument7 SeitenApproach To The PX With CancerSeff CausapinNoch keine Bewertungen
- Abdomen Physical DiagnosisDokument3 SeitenAbdomen Physical DiagnosisSeff CausapinNoch keine Bewertungen
- Disorders of The MediastinumDokument1 SeiteDisorders of The MediastinumSeff CausapinNoch keine Bewertungen
- Peripheral Vascular System Physical DiagnosisDokument3 SeitenPeripheral Vascular System Physical DiagnosisSeff Causapin100% (1)
- Musculoskeletal System Physical DiagnosisDokument4 SeitenMusculoskeletal System Physical DiagnosisSeff Causapin100% (1)
- Disturbances in Respiratory FunctionDokument6 SeitenDisturbances in Respiratory FunctionSeff CausapinNoch keine Bewertungen
- Physical Diagnosis of The ThoraxDokument3 SeitenPhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- Tubulointerstitial DsesDokument3 SeitenTubulointerstitial DsesSeff CausapinNoch keine Bewertungen
- Physical Diagnosis of Cardiovascular SystemDokument6 SeitenPhysical Diagnosis of Cardiovascular SystemSeff Causapin100% (1)
- Pathophysiology of SLEDokument16 SeitenPathophysiology of SLESeff CausapinNoch keine Bewertungen
- Sympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Dokument3 SeitenSympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Seff Causapin100% (1)
- Clinicopathologic Narrative ReportDokument3 SeitenClinicopathologic Narrative ReportSeff CausapinNoch keine Bewertungen
- Salmon Ellos IsDokument3 SeitenSalmon Ellos IsSeff CausapinNoch keine Bewertungen
- LeptospirosisDokument2 SeitenLeptospirosisSeff CausapinNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Guidelines For The Evaluation of Probiotics in FoodDokument11 SeitenGuidelines For The Evaluation of Probiotics in Foodkadec100% (1)
- Past Continuous and Past Simple ExercisesDokument3 SeitenPast Continuous and Past Simple ExercisesAna MateusNoch keine Bewertungen
- Ef6oano Inglesbasico 180711024501 PDFDokument128 SeitenEf6oano Inglesbasico 180711024501 PDFfilipamineiroNoch keine Bewertungen
- Unitized Group RationsDokument12 SeitenUnitized Group RationsArthur BarieNoch keine Bewertungen
- Middlebay Corporation Case StudyDokument4 SeitenMiddlebay Corporation Case StudyVince KechNoch keine Bewertungen
- Write The Plural of The Following Nouns.: Write The Correct Pronoun According To The SentenceDokument5 SeitenWrite The Plural of The Following Nouns.: Write The Correct Pronoun According To The SentenceHenry Arias SolizNoch keine Bewertungen
- Understanding Marketing's Role in Customer InsightsDokument15 SeitenUnderstanding Marketing's Role in Customer InsightsNimal De silvaNoch keine Bewertungen
- What Are Polysaccharides How To ClassifyDokument6 SeitenWhat Are Polysaccharides How To ClassifyBiochemistry DenNoch keine Bewertungen
- Rajni Verma's Diet PlanDokument2 SeitenRajni Verma's Diet PlanPiyushNoch keine Bewertungen
- MAg SPRING 2015 P 4Dokument1 SeiteMAg SPRING 2015 P 4Wallace SinclairNoch keine Bewertungen
- Nutri LiteDokument78 SeitenNutri LiteJuanNoch keine Bewertungen
- Managing Sows and Litters for Healthy Pig GrowthDokument4 SeitenManaging Sows and Litters for Healthy Pig GrowthJaycelle IsubolNoch keine Bewertungen
- Report ScriptDokument4 SeitenReport ScriptLexisNoch keine Bewertungen
- Allrecipes - June-July 2022 USDokument100 SeitenAllrecipes - June-July 2022 USÉva TőkésNoch keine Bewertungen
- Insdag Report PDFDokument51 SeitenInsdag Report PDFJay ParmarNoch keine Bewertungen
- Transparency in Food Supply Chains A Review of Enabling Technology SolutionsDokument8 SeitenTransparency in Food Supply Chains A Review of Enabling Technology SolutionsAnkitNoch keine Bewertungen
- Final Exam - Week 8 English II Group 1Dokument13 SeitenFinal Exam - Week 8 English II Group 1Marcela Marín0% (1)
- Cho Session DesignDokument8 SeitenCho Session DesignConsolacion Binarao DoloresNoch keine Bewertungen
- Chapter 1Dokument18 SeitenChapter 1Enis RachmawatiNoch keine Bewertungen
- BANYUWANGI PRICELIST (Periode 15-20 Mar 2021) SKU Code Nama Barang Harga JualDokument6 SeitenBANYUWANGI PRICELIST (Periode 15-20 Mar 2021) SKU Code Nama Barang Harga JualMas FiNoch keine Bewertungen
- Book Extension Activity - Chocolate Milk Por FavorDokument2 SeitenBook Extension Activity - Chocolate Milk Por Favorapi-534305086Noch keine Bewertungen
- Modul 05 PDFDokument20 SeitenModul 05 PDFNurul Akbar Al-Ghifari 4Noch keine Bewertungen
- Benjamín Flores Castro (Triptico)Dokument2 SeitenBenjamín Flores Castro (Triptico)Sergio Illimani FloresNoch keine Bewertungen
- CLASSIFYING CARBS AND NUTRIENTS FOR ENERGY AND HEALTHDokument52 SeitenCLASSIFYING CARBS AND NUTRIENTS FOR ENERGY AND HEALTHAnna SantosNoch keine Bewertungen
- Refrigerator Cooling and Storage EssentialsDokument20 SeitenRefrigerator Cooling and Storage EssentialsSanjay VermaNoch keine Bewertungen
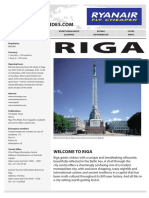
- Riga Travel Guide (2007) by RyanairDokument10 SeitenRiga Travel Guide (2007) by RyanairisrgffNoch keine Bewertungen
- Terminologies, Cooking Methods and TechniquesDokument200 SeitenTerminologies, Cooking Methods and TechniquesAle Grace100% (1)
- Exercise 8 Life SienceDokument2 SeitenExercise 8 Life SienceAndré StrevelNoch keine Bewertungen
- EXPO Report Sustainability ING Rev2014 PDFDokument200 SeitenEXPO Report Sustainability ING Rev2014 PDFBruno Manuel dos Anjos Marques AlbanoNoch keine Bewertungen
- When He Comes, Close Your Eyes PDFDokument613 SeitenWhen He Comes, Close Your Eyes PDFRiza Alvarez93% (14)