Das könnte Ihnen auch gefallen
- An Overview of Removable Partial DentureDokument7 SeitenAn Overview of Removable Partial DenturePatra PrimadanaNoch keine Bewertungen
- Major ConnectorsDokument9 SeitenMajor ConnectorsAyeshaNoch keine Bewertungen
- Precision Attachments Applications and LimitationsDokument9 SeitenPrecision Attachments Applications and LimitationsVivek ShankarNoch keine Bewertungen
- Fixed Orthodontic Appliances: A Practical GuideVon EverandFixed Orthodontic Appliances: A Practical GuideBewertung: 1 von 5 Sternen1/5 (1)
- Clinical Cases in Restorative and Reconstructive DentistryVon EverandClinical Cases in Restorative and Reconstructive DentistryBewertung: 5 von 5 Sternen5/5 (1)
- The Complete Guide To Dentures: All About DentistryVon EverandThe Complete Guide To Dentures: All About DentistryNoch keine Bewertungen
- The Complete Guide to Dental Implants: All About DentistryVon EverandThe Complete Guide to Dental Implants: All About DentistryNoch keine Bewertungen
- Evaluation of Patient in FPDDokument131 SeitenEvaluation of Patient in FPDLucky SinganamalaNoch keine Bewertungen
- 1 Objectives and Classification PD FayadDokument25 Seiten1 Objectives and Classification PD FayadMostafa FayadNoch keine Bewertungen
- Centric Relation PDFDokument3 SeitenCentric Relation PDFrekabiNoch keine Bewertungen
- ProsthoDokument59 SeitenProsthoramNoch keine Bewertungen
- Centric RelationDokument21 SeitenCentric RelationAatish Dilip ShahNoch keine Bewertungen
- DentigenicsinCompleteDentureProsthodontics PDFDokument106 SeitenDentigenicsinCompleteDentureProsthodontics PDFankitaNoch keine Bewertungen
- ConnectorsDokument24 SeitenConnectorsVikas Aggarwal100% (1)
- The Hollow Maxillary Complete DentureDokument24 SeitenThe Hollow Maxillary Complete DentureMahjuba ZehraNoch keine Bewertungen
- Fiber Reinforced CompositeDokument5 SeitenFiber Reinforced Compositejcali06Noch keine Bewertungen
- (Year 3) Removable Prosthodontics Practical - Indirect RetainersDokument6 Seiten(Year 3) Removable Prosthodontics Practical - Indirect Retainerstae hyungNoch keine Bewertungen
- Management of The Soft Palate Defect Steven Eckert PDFDokument15 SeitenManagement of The Soft Palate Defect Steven Eckert PDFintanursamsiNoch keine Bewertungen
- Impressions For FPDDokument53 SeitenImpressions For FPDpragatiNoch keine Bewertungen
- Sri Guru Ram Das Institute of Dental Sciences & Research Sri AmritsarDokument60 SeitenSri Guru Ram Das Institute of Dental Sciences & Research Sri AmritsarKomal SaroyaNoch keine Bewertungen
- Parts & Design of RPDDokument18 SeitenParts & Design of RPDR KaranNoch keine Bewertungen
- Diagnosis of CDDokument79 SeitenDiagnosis of CDAbdelrahman GalalNoch keine Bewertungen
- Imaging in Periodontics PerioDokument49 SeitenImaging in Periodontics PerioFourthMolar.comNoch keine Bewertungen
- Impression TechniqueDokument18 SeitenImpression TechniqueYashpreetsingh BhatiaNoch keine Bewertungen
- Single Complete DentureDokument23 SeitenSingle Complete DentureNelly SuriamahNoch keine Bewertungen
- Dental AnesthesiaDokument20 SeitenDental AnesthesiaAnonymous gUjimJKNoch keine Bewertungen
- Occlusion in Complete DentureDokument20 SeitenOcclusion in Complete DentureBhushan ChavanNoch keine Bewertungen
- Examination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsDokument73 SeitenExamination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsMohamedNoch keine Bewertungen
- Complete Denture TechniquesDokument6 SeitenComplete Denture TechniquesJohn Hyunuk ChoNoch keine Bewertungen
- Journal Club No 1Dokument43 SeitenJournal Club No 1DrBrajendra Singh TomarNoch keine Bewertungen
- Extraction: Department of Oral and Maxillofacial SurgeryDokument26 SeitenExtraction: Department of Oral and Maxillofacial SurgerySudip ChakrabortyNoch keine Bewertungen
- Treatment of Grossly Resorbed Mandibular Ridge 1Dokument48 SeitenTreatment of Grossly Resorbed Mandibular Ridge 1Faheemuddin Muhammad0% (1)
- Overdenture 140503222227 Phpapp01Dokument107 SeitenOverdenture 140503222227 Phpapp01TatsamYadavNoch keine Bewertungen
- Balanced Occlu HandoutDokument9 SeitenBalanced Occlu HandoutMostafa FayadNoch keine Bewertungen
- Anatomical Landmarks of MaxillaDokument51 SeitenAnatomical Landmarks of MaxillaPadma GnanamNoch keine Bewertungen
- Prostho 9, Teeth SettingDokument15 SeitenProstho 9, Teeth SettingJustDen09Noch keine Bewertungen
- Combination Syndrome PDFDokument5 SeitenCombination Syndrome PDFfirginaaNoch keine Bewertungen
- Open-Cap Acrylic SplintDokument3 SeitenOpen-Cap Acrylic SplintFeras Al-ZbounNoch keine Bewertungen
- Removable Prosthodontics II - Lec.7, Minor Connectors - SIUST, College of DentistyDokument4 SeitenRemovable Prosthodontics II - Lec.7, Minor Connectors - SIUST, College of DentistyNoor Al-Deen Maher0% (1)
- Pontic SDokument52 SeitenPontic SLalit Kumar100% (2)
- Posterior Palatal Seal AreaDokument8 SeitenPosterior Palatal Seal Areaayan ravalNoch keine Bewertungen
- Finish LinesDokument17 SeitenFinish LinesWaseem AhmedNoch keine Bewertungen
- Retention Support Stability CDDokument53 SeitenRetention Support Stability CDAshraf GebreelNoch keine Bewertungen
- AnthropometricDokument11 SeitenAnthropometricdrrebaNoch keine Bewertungen
- Mouth Preperation RPDDokument14 SeitenMouth Preperation RPDSadishNoch keine Bewertungen
- Stress Treatment Theorem For Implant Dentistry: Niranjana R I Year Postgraduate Department of ProsthodonticsDokument43 SeitenStress Treatment Theorem For Implant Dentistry: Niranjana R I Year Postgraduate Department of ProsthodonticsNiranjanaNoch keine Bewertungen
- Occlusion in RPDDokument5 SeitenOcclusion in RPDDhananjay GandageNoch keine Bewertungen
- JInterdiscipDentistry3112-5456729 150927Dokument6 SeitenJInterdiscipDentistry3112-5456729 150927Nisha GargNoch keine Bewertungen
- Principles of Removable Partial Denture DesignDokument7 SeitenPrinciples of Removable Partial Denture DesignAls EchanoNoch keine Bewertungen
- Incisal GuidanceDokument5 SeitenIncisal Guidancejinny1_0Noch keine Bewertungen
- Rehabilitation of Maxillary DefecysDokument67 SeitenRehabilitation of Maxillary DefecyspriyaNoch keine Bewertungen
- Indian Dental Academy - Theories of Impression Making in Complete Denture Treatment PDFDokument15 SeitenIndian Dental Academy - Theories of Impression Making in Complete Denture Treatment PDFFaheemuddin MuhammadNoch keine Bewertungen
- Management of Perio Prostho Situations in DentistryDokument18 SeitenManagement of Perio Prostho Situations in DentistryHarsha ReddyNoch keine Bewertungen
- A Review of The Success and Failure Characteristics of Resin-Bonded BridgesDokument10 SeitenA Review of The Success and Failure Characteristics of Resin-Bonded BridgesMichael XuNoch keine Bewertungen
- Lec1 - Bridge (Fixed Partial DentureDokument9 SeitenLec1 - Bridge (Fixed Partial Dentureكاظم عبد الحسينNoch keine Bewertungen
- Concept: Captek™ Are Crowns and Bridges That Mimic and Surpass Natural Teeth in Esthetic and FunctionDokument50 SeitenConcept: Captek™ Are Crowns and Bridges That Mimic and Surpass Natural Teeth in Esthetic and FunctionPolet Aline Sánchez SosaNoch keine Bewertungen
- Anomalies of The Orofacial RegionDokument118 SeitenAnomalies of The Orofacial RegionAhmed Barakat100% (1)
- Recent Advances in Procthodontics - LD (AMAR)Dokument102 SeitenRecent Advances in Procthodontics - LD (AMAR)Archana PanwarNoch keine Bewertungen
- Type I: Luting Agents That Include Permanent and Temporary Cements. Type II: Restorative Applications. Type III: Liner or Base ApplicationsDokument5 SeitenType I: Luting Agents That Include Permanent and Temporary Cements. Type II: Restorative Applications. Type III: Liner or Base ApplicationsSony RajbhandariNoch keine Bewertungen
- Management of Medical Emergencies in The Dental OfficeDokument38 SeitenManagement of Medical Emergencies in The Dental OfficeJohan Edward Franklin MarpaungNoch keine Bewertungen
- NewpinyinDokument30 SeitenNewpinyinJohn Albert NajesNoch keine Bewertungen
- Gupta Swati Quick Review Ä°n Clinical Periodontics 01Dokument1 SeiteGupta Swati Quick Review Ä°n Clinical Periodontics 01Vincent SerNoch keine Bewertungen
- Syndromes of The Head and Neck - An Issue of Atlas of The Oral & Maxillofacial Surgery Clinics (The Clinics - Dentistry) (2014) (UnitedVRG)Dokument132 SeitenSyndromes of The Head and Neck - An Issue of Atlas of The Oral & Maxillofacial Surgery Clinics (The Clinics - Dentistry) (2014) (UnitedVRG)Darryl Villar100% (4)
- Learning Chinese: A Foundation Course IN MandarinDokument135 SeitenLearning Chinese: A Foundation Course IN MandarinDos-peter John Bilbao87% (15)
- A Beginner's Guide To Starting An Import - Export Business With ChinaDokument8 SeitenA Beginner's Guide To Starting An Import - Export Business With ChinaVincent SerNoch keine Bewertungen
- Case HistoryDokument50 SeitenCase HistoryVincent SerNoch keine Bewertungen
- Orthopedics & FracturesDokument45 SeitenOrthopedics & FracturesVincent SerNoch keine Bewertungen
- Exodontia in Pediatric Dental Patient: 1 Pediatrics For Dentistry C-IDokument50 SeitenExodontia in Pediatric Dental Patient: 1 Pediatrics For Dentistry C-IVincent SerNoch keine Bewertungen
- Composite RestorationDokument54 SeitenComposite RestorationVincent SerNoch keine Bewertungen
- Diagnosis and Treatment PlanningDokument66 SeitenDiagnosis and Treatment PlanningVincent SerNoch keine Bewertungen
- Seminar Planning: On FamilyDokument3 SeitenSeminar Planning: On FamilyVincent SerNoch keine Bewertungen
- Methods of Space GainingDokument95 SeitenMethods of Space GainingVincent Ser100% (4)
- Early Childhood CariesDokument20 SeitenEarly Childhood CariesVincent SerNoch keine Bewertungen
- Childhood TuberculosisDokument59 SeitenChildhood TuberculosisVincent SerNoch keine Bewertungen
- All - Ceramic Restorations: Composition of Ceramic Products Based On Feldspar, Kaolin and QuartzDokument9 SeitenAll - Ceramic Restorations: Composition of Ceramic Products Based On Feldspar, Kaolin and QuartzVincent Ser100% (1)
- Drugs in PeriodontologyDokument68 SeitenDrugs in PeriodontologyVincent SerNoch keine Bewertungen
- Endo EmergenciesDokument95 SeitenEndo EmergenciesVincent SerNoch keine Bewertungen
- Diseases of Dental Pulp and Peri Radicular TissuesDokument69 SeitenDiseases of Dental Pulp and Peri Radicular TissuesVincent SerNoch keine Bewertungen
- Impression MakingDokument14 SeitenImpression MakingVincent SerNoch keine Bewertungen
- Surgical Aspects of Pulmonary Infections: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDokument60 SeitenSurgical Aspects of Pulmonary Infections: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNoch keine Bewertungen
- Mediastinal Tumors: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDokument52 SeitenMediastinal Tumors: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNoch keine Bewertungen
- Mediastinal Tumors: by Temesgen G/MariamDokument51 SeitenMediastinal Tumors: by Temesgen G/MariamVincent SerNoch keine Bewertungen
- Surgical Conditions of Pleura: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDokument63 SeitenSurgical Conditions of Pleura: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNoch keine Bewertungen
- Pulmonary Complications of HIVDokument43 SeitenPulmonary Complications of HIVVincent SerNoch keine Bewertungen
- Vascular Diseases: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDokument57 SeitenVascular Diseases: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNoch keine Bewertungen
- Esophageal Conditions: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDokument54 SeitenEsophageal Conditions: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNoch keine Bewertungen
- Intestinal Obstruction: Yohannes TDokument34 SeitenIntestinal Obstruction: Yohannes TVincent Ser100% (1)
- Diabetus MellitusDokument74 SeitenDiabetus MellitusVincent SerNoch keine Bewertungen
- TutorialDokument29 SeitenTutorialVilza maharaniNoch keine Bewertungen
- Tan, Jolwin Laugo 2361052561Dokument6 SeitenTan, Jolwin Laugo 2361052561JolwinTanNoch keine Bewertungen
- Exporters DirectoryDokument1 SeiteExporters DirectoryMipta KurniawanNoch keine Bewertungen
- WonderlandDokument2 SeitenWonderlandJohn WilliamsNoch keine Bewertungen
- CrocodilesDokument3 SeitenCrocodilesPeculiarMemoriesNoch keine Bewertungen
- Mollusks & EchinodermDokument18 SeitenMollusks & EchinodermRoselle GuevaraNoch keine Bewertungen
- Chhiarpui Neih Tan A Ni: Hunawl Hman That Zofate Hmasawnna Ngaihtuah Kriastian Nun Dan Tha NgaihsanDokument4 SeitenChhiarpui Neih Tan A Ni: Hunawl Hman That Zofate Hmasawnna Ngaihtuah Kriastian Nun Dan Tha NgaihsanchanmariansNoch keine Bewertungen
- Medical-Surgical Nursing Exam 7 (25 Items)Dokument4 SeitenMedical-Surgical Nursing Exam 7 (25 Items)lovely_omegaNoch keine Bewertungen
- NEF PRE-int UNIT 1Dokument11 SeitenNEF PRE-int UNIT 1Ma Gabriela Ojeda CasellaNoch keine Bewertungen
- Dragonix - DM Options, Monster Talents IIDokument246 SeitenDragonix - DM Options, Monster Talents IIJolticsy Rules100% (8)
- Fun 2nd Grade Math WorksheetDokument4 SeitenFun 2nd Grade Math WorksheetAtri NadiaNoch keine Bewertungen
- Y 0870 e 51Dokument12 SeitenY 0870 e 51Yohanes BaptistaNoch keine Bewertungen
- ENGLISHDokument5 SeitenENGLISHRashmia LacsonNoch keine Bewertungen
- Cat and Mouse 2Dokument2 SeitenCat and Mouse 2Da MiánNoch keine Bewertungen
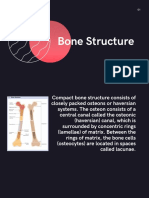
- Topic PPT Bone StructureDokument14 SeitenTopic PPT Bone StructureMoonNoch keine Bewertungen
- The ScarecrowDokument5 SeitenThe ScarecrowJuvent0% (1)
- Articles, Determiners & Quantifiers Set 1Dokument25 SeitenArticles, Determiners & Quantifiers Set 1fatoNoch keine Bewertungen
- DND 5e Races and SubracesDokument3 SeitenDND 5e Races and SubracesCursedLich89% (9)
- Types of Reproduction: Sexual AsexualDokument45 SeitenTypes of Reproduction: Sexual AsexualasdNoch keine Bewertungen
- ENGLISH (Core) : Series OSR/1/CDokument11 SeitenENGLISH (Core) : Series OSR/1/CarjunNoch keine Bewertungen
- GG BA Honours Semester 2 Ode On The Death of A Favourite Cat Lecture 1Dokument15 SeitenGG BA Honours Semester 2 Ode On The Death of A Favourite Cat Lecture 1archana anilNoch keine Bewertungen
- Developing The Straight Body Cast To HandstandDokument6 SeitenDeveloping The Straight Body Cast To HandstandValentin Uzunov100% (1)
- Reading SMPDokument43 SeitenReading SMPSharah RahmawatiNoch keine Bewertungen
- Aulia Rahmatun Nufus Raihanun Nisa Dinur Sri RizkiDokument18 SeitenAulia Rahmatun Nufus Raihanun Nisa Dinur Sri RizkiFauzan JakfarNoch keine Bewertungen
- Small Pox Is DeadDokument46 SeitenSmall Pox Is Deadtummalapalli venkateswara raoNoch keine Bewertungen
- Mixed Dentition AnalysisDokument6 SeitenMixed Dentition AnalysisJess JesiNoch keine Bewertungen
- Dodram Handon - 2016 (Dodram Food)Dokument13 SeitenDodram Handon - 2016 (Dodram Food)wong winkinNoch keine Bewertungen
- HAYDUKE, George - ''Make'Em Pay - Ultimate Revenge Techniques From The Master Trickster''Dokument125 SeitenHAYDUKE, George - ''Make'Em Pay - Ultimate Revenge Techniques From The Master Trickster''Mitko Krumov100% (3)
- Sale Catalog - World Classic SaleDokument52 SeitenSale Catalog - World Classic SaleHolstein PlazaNoch keine Bewertungen
- The Wax # 9Dokument54 SeitenThe Wax # 9Emmanuel MilwaukeeNoch keine Bewertungen