Das könnte Ihnen auch gefallen
- Salvador Minuchin On Family Therapy: Instructor'S ManualDokument48 SeitenSalvador Minuchin On Family Therapy: Instructor'S ManualAisyah Zulkepli100% (1)
- A Connection Between A Symbol and A SymptomDokument1 SeiteA Connection Between A Symbol and A SymptomBasil LipcanNoch keine Bewertungen
- Manual 24 Hour RecallDokument160 SeitenManual 24 Hour RecallMadalina CervidNoch keine Bewertungen
- 8 Part Eye Exam RevisedDokument17 Seiten8 Part Eye Exam RevisedpasambalyrradjohndarNoch keine Bewertungen
- 8 Part Eye Exam RevisedDokument17 Seiten8 Part Eye Exam RevisedpasambalyrradjohndarNoch keine Bewertungen
- Rape Trauma Syndrome NCPDokument5 SeitenRape Trauma Syndrome NCPMarife Lipana Reyes67% (3)
- Icd 9 CMDokument3 SeitenIcd 9 CMRetno75% (8)
- "The Amrut in Dehydration": Paediatrics Department VMMC & H, KaraikalDokument38 Seiten"The Amrut in Dehydration": Paediatrics Department VMMC & H, KaraikalSumanth KumarNoch keine Bewertungen
- Oral Rehydration TherapyDokument17 SeitenOral Rehydration TherapyJaya PrabhaNoch keine Bewertungen
- Different Types of IV FluidsDokument6 SeitenDifferent Types of IV FluidsnicoleNoch keine Bewertungen
- CVP MonitoringDokument24 SeitenCVP MonitoringChoji Heiwajima100% (1)
- Florence Nightingale's Environmental Theory: Josephine Ann J. Necor, RNDokument38 SeitenFlorence Nightingale's Environmental Theory: Josephine Ann J. Necor, RNBheru LalNoch keine Bewertungen
- Ferrous Sulfate: Generic NameDokument3 SeitenFerrous Sulfate: Generic NamefahadNoch keine Bewertungen
- NEPHROSISDokument31 SeitenNEPHROSISvinnu kalyanNoch keine Bewertungen
- Breast Pumps: PRESENTED BY: Shristi PanthaDokument16 SeitenBreast Pumps: PRESENTED BY: Shristi PanthaShristi PanthaNoch keine Bewertungen
- Vitamin Deficiency DisordersDokument23 SeitenVitamin Deficiency DisordersKibromWeldegiyorgisNoch keine Bewertungen
- Liver Transplant - PedsDokument15 SeitenLiver Transplant - Pedsbencleese100% (2)
- Oral Rehydration TherapyDokument42 SeitenOral Rehydration TherapyGaurav GuptaNoch keine Bewertungen
- Practical 2 Administration of Nursing/Clinical Unit: Tructu eDokument12 SeitenPractical 2 Administration of Nursing/Clinical Unit: Tructu eElizabath XavierNoch keine Bewertungen
- Iv TherapyDokument3 SeitenIv TherapylovlyNoch keine Bewertungen
- Central Venous PressureDokument10 SeitenCentral Venous PressureAngelo ArquizaNoch keine Bewertungen
- DehydrationDokument16 SeitenDehydrationBenben LookitandI'mNoch keine Bewertungen
- Health Assessment of Bronchial Asthma PatientDokument3 SeitenHealth Assessment of Bronchial Asthma PatientShetal SharmaNoch keine Bewertungen
- DialysisDokument3 SeitenDialysisSarah BenjaminNoch keine Bewertungen
- Medscape Status EpilepticusDokument10 SeitenMedscape Status EpilepticusEllen Siska SusantiNoch keine Bewertungen
- Seminar 2 Endocrine DisordersDokument44 SeitenSeminar 2 Endocrine DisordersSuganthi ParthibanNoch keine Bewertungen
- Oral Rehydration Salt (Ors)Dokument2 SeitenOral Rehydration Salt (Ors)Bijaya BhattaNoch keine Bewertungen
- PBBN 1St Yr Child Health Nursing CBIMNCIDokument29 SeitenPBBN 1St Yr Child Health Nursing CBIMNCIcopy smart100% (1)
- DialysisDokument20 SeitenDialysisSiwani rai100% (1)
- Enteric FeverDokument51 SeitenEnteric FeverBinayaNoch keine Bewertungen
- Different Types of OrsDokument26 SeitenDifferent Types of Orsapi-382378575% (4)
- The Benefits of Donating Blood: October 2017Dokument10 SeitenThe Benefits of Donating Blood: October 2017MAHESH KOUJALAGINoch keine Bewertungen
- Alternative System of MedicineDokument38 SeitenAlternative System of MedicineshijuvarghesepgNoch keine Bewertungen
- Cpms College of Nursing: Assignment ON Colonic IrrigationDokument3 SeitenCpms College of Nursing: Assignment ON Colonic IrrigationAmy Lalringhluani ChhakchhuakNoch keine Bewertungen
- Seizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HDokument70 SeitenSeizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HRohini RaiNoch keine Bewertungen
- Liver Function Test FinalDokument98 SeitenLiver Function Test FinalHussain AzharNoch keine Bewertungen
- ANAMEIA PPT BY SandeepDokument32 SeitenANAMEIA PPT BY SandeepSandeep ChakravarthyNoch keine Bewertungen
- TI M E Contrib Utory Objecti VE Content Teaching Learning Activity A.V.Aids Evalua-TionDokument11 SeitenTI M E Contrib Utory Objecti VE Content Teaching Learning Activity A.V.Aids Evalua-TionBinal JoshiNoch keine Bewertungen
- Acute Kidney FailureDokument8 SeitenAcute Kidney Failureanimesh pandaNoch keine Bewertungen
- N7 by Novo - Methods of ContraceptionDokument34 SeitenN7 by Novo - Methods of ContraceptionEllen Rose NovoNoch keine Bewertungen
- Gastrostomy FeedingDokument9 SeitenGastrostomy FeedingJovil PajaronNoch keine Bewertungen
- FundosDokument13 SeitenFundosLi FaungNoch keine Bewertungen
- Poisoning DecontaminationDokument14 SeitenPoisoning DecontaminationadystiNoch keine Bewertungen
- Oxygen Therapy and Oxygen Delivery (Pediatric) - CEDokument8 SeitenOxygen Therapy and Oxygen Delivery (Pediatric) - CEViviana AltamiranoNoch keine Bewertungen
- Stomal TherapyDokument2 SeitenStomal Therapyসায়ন্তন দত্ত100% (1)
- Nursing Practice Standards2Dokument25 SeitenNursing Practice Standards2sunielgowdaNoch keine Bewertungen
- Levels of PreventionDokument12 SeitenLevels of PreventionRuth EkanemNoch keine Bewertungen
- Bowel TrainingDokument2 SeitenBowel Trainingdickie.gdrNoch keine Bewertungen
- NephritisDokument21 SeitenNephritisruchikaNoch keine Bewertungen
- Cystic FibrosisDokument2 SeitenCystic FibrosisYanyan Umpar PologNoch keine Bewertungen
- Cardiac EmergenciesDokument73 SeitenCardiac EmergenciesKristine CaringalNoch keine Bewertungen
- DR Soni Rani, PGT Katihar Medical College, KatiharDokument59 SeitenDR Soni Rani, PGT Katihar Medical College, KatiharRamniwasMahoreNoch keine Bewertungen
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDokument12 SeitenMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RNoch keine Bewertungen
- Changing Trend in Hospitalization Old ConceptsDokument8 SeitenChanging Trend in Hospitalization Old ConceptsMakhanVermaNoch keine Bewertungen
- CVPDokument23 SeitenCVPShalini KaluraNoch keine Bewertungen
- Universal PrecautionDokument10 SeitenUniversal PrecautionParth VasaveNoch keine Bewertungen
- Arterial Blood PressureDokument21 SeitenArterial Blood PressureMaham SaleemNoch keine Bewertungen
- Diarrhea: DEFINITION-Diarrhea Is Define As The Passage of Loose, Liquid orDokument6 SeitenDiarrhea: DEFINITION-Diarrhea Is Define As The Passage of Loose, Liquid orNiharika ChauhanNoch keine Bewertungen
- Link ClickDokument4 SeitenLink ClickMitch MontielNoch keine Bewertungen
- Immunisation ScheduleDokument3 SeitenImmunisation SchedulejegathesmsjsNoch keine Bewertungen
- Fluid and Electrolyte Imbalance and Nutritional ProblemDokument98 SeitenFluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerNoch keine Bewertungen
- Viral Hepatitis: Dr. Khaled JadallahDokument24 SeitenViral Hepatitis: Dr. Khaled JadallahRashed ShatnawiNoch keine Bewertungen
- TyphoidDokument10 SeitenTyphoidpeterjongNoch keine Bewertungen
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Dokument13 SeitenSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanNoch keine Bewertungen
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesVon EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- (PHA) 2.01 Anti-Muscarinics-Dr - ReyesDokument8 Seiten(PHA) 2.01 Anti-Muscarinics-Dr - ReyespasambalyrradjohndarNoch keine Bewertungen
- (PHA) 4.01 Respiratory Antimicrobials - Dr. de La Cruz v3Dokument16 Seiten(PHA) 4.01 Respiratory Antimicrobials - Dr. de La Cruz v3pasambalyrradjohndarNoch keine Bewertungen
- (EPI) 2nd LE Cup Noodles 2021C PDFDokument5 Seiten(EPI) 2nd LE Cup Noodles 2021C PDFpasambalyrradjohndarNoch keine Bewertungen
- Psych Osce Reviewer 1Dokument10 SeitenPsych Osce Reviewer 1pasambalyrradjohndarNoch keine Bewertungen
- (PHA) 2.13 Immunopharmacology - Dr. Marbella PDFDokument10 Seiten(PHA) 2.13 Immunopharmacology - Dr. Marbella PDFpasambalyrradjohndarNoch keine Bewertungen
- (PHA) 2.10c Anti-Hansens Agents - Dr. Macaraig PDFDokument3 Seiten(PHA) 2.10c Anti-Hansens Agents - Dr. Macaraig PDFpasambalyrradjohndarNoch keine Bewertungen
- OSCE Must Knows For All SubjectsDokument8 SeitenOSCE Must Knows For All SubjectsPrincess Jeanne Roque GairanodNoch keine Bewertungen
- Application For Academic RecordDokument1 SeiteApplication For Academic RecordpasambalyrradjohndarNoch keine Bewertungen
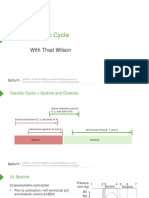
- Cardiac Cycle: With Thad WilsonDokument25 SeitenCardiac Cycle: With Thad WilsonpasambalyrradjohndarNoch keine Bewertungen
- Cardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DDokument36 SeitenCardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DpasambalyrradjohndarNoch keine Bewertungen
- (PHA) 2.12 Anti-Fungal Agents - Dr. Cabreros PDFDokument7 Seiten(PHA) 2.12 Anti-Fungal Agents - Dr. Cabreros PDFpasambalyrradjohndarNoch keine Bewertungen
- (PHA) 2.11 Anti-Viral Drugs - Dr. Cacayorin PDFDokument15 Seiten(PHA) 2.11 Anti-Viral Drugs - Dr. Cacayorin PDFpasambalyrradjohndar0% (1)
- Monthly Blood Glucose Diary PDFDokument1 SeiteMonthly Blood Glucose Diary PDFpasambalyrradjohndarNoch keine Bewertungen
- Loop Diuretics: Producers of The Greatest Diuresis With Rhonda LawesDokument23 SeitenLoop Diuretics: Producers of The Greatest Diuresis With Rhonda LawespasambalyrradjohndarNoch keine Bewertungen
- Cpm15th Dengue Fever (Doh)Dokument18 SeitenCpm15th Dengue Fever (Doh)Jeanne Marie ValesNoch keine Bewertungen
- Working With Children With Cleft Lip and PalateDokument27 SeitenWorking With Children With Cleft Lip and PalateMarcus Skookumchuck VanniniNoch keine Bewertungen
- EBM and CAT - General Instructions For 2019-2020Dokument2 SeitenEBM and CAT - General Instructions For 2019-2020pasambalyrradjohndarNoch keine Bewertungen
- Cardiac Mechanics: With Thad WilsonDokument26 SeitenCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNoch keine Bewertungen
- Gastric CancerDokument15 SeitenGastric Cancerisaco1531012Noch keine Bewertungen
- (CLINPATH) 2.02 Transfusion II - Dr.-VillamayorDokument7 Seiten(CLINPATH) 2.02 Transfusion II - Dr.-VillamayorpasambalyrradjohndarNoch keine Bewertungen
- Recording The Medical HistoryDokument8 SeitenRecording The Medical HistorypasambalyrradjohndarNoch keine Bewertungen
- OSCE Must Knows For All SubjectsDokument8 SeitenOSCE Must Knows For All SubjectsPrincess Jeanne Roque GairanodNoch keine Bewertungen
- Psych Osce Reviewer 1Dokument10 SeitenPsych Osce Reviewer 1pasambalyrradjohndarNoch keine Bewertungen
- Cis 2018Dokument1 SeiteCis 2018pasambalyrradjohndarNoch keine Bewertungen
- (MICRO) 2.03 Acid Fast StainingDokument2 Seiten(MICRO) 2.03 Acid Fast Stainingpasambalyrradjohndar0% (1)
- Psych Osce Reviewer 1Dokument10 SeitenPsych Osce Reviewer 1pasambalyrradjohndarNoch keine Bewertungen
- Cis 2018 PDFDokument3 SeitenCis 2018 PDFTara Oliveros Dela CruzNoch keine Bewertungen
- A Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmciDokument3 SeitenA Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmcipasambalyrradjohndarNoch keine Bewertungen
- Theoretical Application of Kohutian Theory To Anorexia and Bulimia NervosaDokument12 SeitenTheoretical Application of Kohutian Theory To Anorexia and Bulimia NervosakelkarinNoch keine Bewertungen
- Nausea and VomitingDokument5 SeitenNausea and VomitingIndra Setya PermanaNoch keine Bewertungen
- Antiprotozoa MedicineDokument10 SeitenAntiprotozoa MedicineWaldian IsmailNoch keine Bewertungen
- The Compassion Fatigue and Resilience Connection A Survey of Resilience Compassion Fatigue Burnout and Compassion Satisfaction Among Trauma Responders 1522 4821 17 165 PDFDokument9 SeitenThe Compassion Fatigue and Resilience Connection A Survey of Resilience Compassion Fatigue Burnout and Compassion Satisfaction Among Trauma Responders 1522 4821 17 165 PDFMarc Andreo MalalaNoch keine Bewertungen
- Obsessive Compulsive Disorder Punjabi Instant Download 1Dokument3 SeitenObsessive Compulsive Disorder Punjabi Instant Download 1Ameera ChauhanNoch keine Bewertungen
- Hydrotherapy Knee OA Exercise SheetDokument6 SeitenHydrotherapy Knee OA Exercise SheetMuhammad Faishal Imam AfifNoch keine Bewertungen
- Inhibitory Activity and Phytochemical Assessment of Ethno-Medicinal Plants Against Some Human Pathogenic BacteriaDokument8 SeitenInhibitory Activity and Phytochemical Assessment of Ethno-Medicinal Plants Against Some Human Pathogenic BacteriaLavanya Priya SathyanNoch keine Bewertungen
- Case Study-Chronic TonsillitisDokument7 SeitenCase Study-Chronic TonsillitisJonalyn TumanguilNoch keine Bewertungen
- Emergency DrugsDokument47 SeitenEmergency DrugsBesimanNoch keine Bewertungen
- BPPVDokument36 SeitenBPPVRizka AmaliaNoch keine Bewertungen
- Hydrocele, Surgery Vs Sclerotherapy JHBHDokument4 SeitenHydrocele, Surgery Vs Sclerotherapy JHBHreeves_coolNoch keine Bewertungen
- Keganasan HematologiDokument26 SeitenKeganasan HematologiRizzal Selviyana SuhardiNoch keine Bewertungen
- Aquatic Therapy Journal Aug 2005 Vol 7Dokument28 SeitenAquatic Therapy Journal Aug 2005 Vol 7Barbu Alexandru StefanNoch keine Bewertungen
- Approaches of CunsellingDokument5 SeitenApproaches of CunsellingNelson Grande CalimagNoch keine Bewertungen
- DentalUpdate March2018Dokument100 SeitenDentalUpdate March2018OTNoch keine Bewertungen
- Birth of CosmopathyDokument7 SeitenBirth of CosmopathyKirti BetaiNoch keine Bewertungen
- Both Positive Mental Health and Psychopathology Should Be Monitored in Psychotherapy Confirmation For The Dual-Factor Model in Acceptance and Commitment Therapy.Dokument24 SeitenBoth Positive Mental Health and Psychopathology Should Be Monitored in Psychotherapy Confirmation For The Dual-Factor Model in Acceptance and Commitment Therapy.Zyan D. RiveraNoch keine Bewertungen
- Cleft Lip / Cleft Palate: Predisposing FactorsDokument15 SeitenCleft Lip / Cleft Palate: Predisposing FactorsMabesNoch keine Bewertungen
- The Skin Is An Organ of ProtectionDokument5 SeitenThe Skin Is An Organ of ProtectionFahmi Sulistyo HutomoNoch keine Bewertungen
- Prostate SmallDokument1 SeiteProstate SmallChintya Permata SariNoch keine Bewertungen
- Exit Site Wounds Made EasyDokument6 SeitenExit Site Wounds Made EasyMimi MuhammidaNoch keine Bewertungen
- Test Bank Chapter 5: Psychosocial Alterations: Urden: Thelan's Critical Care Nursing, 5 EditionDokument8 SeitenTest Bank Chapter 5: Psychosocial Alterations: Urden: Thelan's Critical Care Nursing, 5 EditionAnonymous ZzjzIcmNoch keine Bewertungen
- Institutional Case PreDokument31 SeitenInstitutional Case PreRiza AcebucheNoch keine Bewertungen
- Restless Leg Syndrome: The Most Common Disorder You Have Never Heard Of."Dokument20 SeitenRestless Leg Syndrome: The Most Common Disorder You Have Never Heard Of."Maulida Manurung100% (1)
- How Does Dependent Personality Disorder Form, Develop and Affect Human Life?Dokument5 SeitenHow Does Dependent Personality Disorder Form, Develop and Affect Human Life?myuniieNoch keine Bewertungen
- Udan's Neuro, Musculoskel, EentDokument2 SeitenUdan's Neuro, Musculoskel, EentReygie Marsada100% (4)