Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- CII Sohrabji Godrej GreenDokument30 SeitenCII Sohrabji Godrej GreenRITHANYAA100% (2)
- Coaxial Cable Attenuation ChartDokument6 SeitenCoaxial Cable Attenuation ChartNam PhamNoch keine Bewertungen
- Case Study - Suprema CarsDokument5 SeitenCase Study - Suprema CarsALFONSO PATRICIO GUERRA CARVAJALNoch keine Bewertungen
- XII CS Material Chap7 2012 13Dokument21 SeitenXII CS Material Chap7 2012 13Ashis PradhanNoch keine Bewertungen
- Immunity Question Paper For A Level BiologyDokument2 SeitenImmunity Question Paper For A Level BiologyJansi Angel100% (1)
- Quality Control of Rigid Pavements 1Dokument58 SeitenQuality Control of Rigid Pavements 1pranjpatil100% (1)
- Practice Problems - Electrochemical CellDokument5 SeitenPractice Problems - Electrochemical CellYehia IbrahimNoch keine Bewertungen
- 19 Dark PPT TemplateDokument15 Seiten19 Dark PPT TemplateKurt W. DelleraNoch keine Bewertungen
- 220245-MSBTE-22412-Java (Unit 1)Dokument40 Seiten220245-MSBTE-22412-Java (Unit 1)Nomaan ShaikhNoch keine Bewertungen
- Loctite 586 PDFDokument9 SeitenLoctite 586 PDForihimieNoch keine Bewertungen
- CH-5 Further Percentages AnswersDokument5 SeitenCH-5 Further Percentages AnswersMaram MohanNoch keine Bewertungen
- Literature Review Template DownloadDokument4 SeitenLiterature Review Template Downloadaflsigfek100% (1)
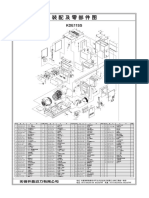
- KDE11SSDokument2 SeitenKDE11SSluisgomezpasion1Noch keine Bewertungen
- APA Vs Harvard Referencing - PDFDokument4 SeitenAPA Vs Harvard Referencing - PDFTalo Contajazz Chileshe50% (2)
- Computer System Validation - Definition and Requirements - MustRead PDFDokument3 SeitenComputer System Validation - Definition and Requirements - MustRead PDFtraining validNoch keine Bewertungen
- KLA28 ProductsapplicationpresetDokument2 SeitenKLA28 ProductsapplicationpresetcarxmozNoch keine Bewertungen
- Project Quality Plan (JFJS-788)Dokument18 SeitenProject Quality Plan (JFJS-788)mominNoch keine Bewertungen
- Introduction CompilerDokument47 SeitenIntroduction CompilerHarshit SinghNoch keine Bewertungen
- LP32HS User Manual v1Dokument52 SeitenLP32HS User Manual v1tonizx7rrNoch keine Bewertungen
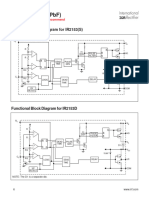
- IR2153 Parte6Dokument1 SeiteIR2153 Parte6FRANK NIELE DE OLIVEIRANoch keine Bewertungen
- The Linguistic Colonialism of EnglishDokument4 SeitenThe Linguistic Colonialism of EnglishAdriana MirandaNoch keine Bewertungen
- Precursor Effects of Citric Acid and Citrates On Zno Crystal FormationDokument7 SeitenPrecursor Effects of Citric Acid and Citrates On Zno Crystal FormationAlv R GraciaNoch keine Bewertungen
- BBL PR Centralizer Rig Crew Handout (R1.1 2-20-19)Dokument2 SeitenBBL PR Centralizer Rig Crew Handout (R1.1 2-20-19)NinaNoch keine Bewertungen
- Jonathan Livingston Seagull - Richard Bach - (SAW000) PDFDokument39 SeitenJonathan Livingston Seagull - Richard Bach - (SAW000) PDFAdrià SonetNoch keine Bewertungen
- SIVACON 8PS - Planning With SIVACON 8PS Planning Manual, 11/2016, A5E01541101-04Dokument1 SeiteSIVACON 8PS - Planning With SIVACON 8PS Planning Manual, 11/2016, A5E01541101-04marcospmmNoch keine Bewertungen
- ADokument54 SeitenActyvteNoch keine Bewertungen
- G2 Rust Grades USA PDFDokument2 SeitenG2 Rust Grades USA PDFSt3fandragos4306Noch keine Bewertungen
- Genil v. Rivera DigestDokument3 SeitenGenil v. Rivera DigestCharmila SiplonNoch keine Bewertungen
- Enlightened ExperimentationDokument8 SeitenEnlightened ExperimentationRaeed HassanNoch keine Bewertungen
- European Asphalt Standards DatasheetDokument1 SeiteEuropean Asphalt Standards DatasheetmandraktreceNoch keine Bewertungen