Das könnte Ihnen auch gefallen
- Block 1Dokument29 SeitenBlock 1Komal BanoNoch keine Bewertungen
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicVon EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicBewertung: 5 von 5 Sternen5/5 (1)
- ObGyn NotesDokument10 SeitenObGyn NotesKumarNoch keine Bewertungen
- Totalizare GynecoDokument10 SeitenTotalizare GynecoCristinaCapros0% (1)
- 17Dokument19 Seiten17Francisco Javier Ortega Guillem0% (1)
- Day 13th October 2023 RecallDokument12 SeitenDay 13th October 2023 RecallprathibaNoch keine Bewertungen
- Gynecologic Neoplasia Topic 1: Gestational Trophoblastic Neoplasia (GTD)Dokument4 SeitenGynecologic Neoplasia Topic 1: Gestational Trophoblastic Neoplasia (GTD)Elaine Marie Rendon PalmejarNoch keine Bewertungen
- Blueprints Obstetrics and Gynecology 5th Edition MCQDokument30 SeitenBlueprints Obstetrics and Gynecology 5th Edition MCQsinglez100% (1)
- Sample Questions For Emstrex 2012Dokument6 SeitenSample Questions For Emstrex 2012Dr.2020100% (1)
- Obstetric ExamDokument35 SeitenObstetric ExamRafi MahandaruNoch keine Bewertungen
- Soal Usulan Unas Unhas November 2018Dokument26 SeitenSoal Usulan Unas Unhas November 2018Umaimah ShahabNoch keine Bewertungen
- Tes PanoramaDokument57 SeitenTes Panoramamuttaqin95Noch keine Bewertungen
- Morning Report CFDokument33 SeitenMorning Report CFdr.ronak1996Noch keine Bewertungen
- Incomplete Miscarriage Finaliiiii 2.0Dokument10 SeitenIncomplete Miscarriage Finaliiiii 2.0emmanuel oduNoch keine Bewertungen
- 2 PLACENTA PREVIA Case PresentationDokument19 Seiten2 PLACENTA PREVIA Case PresentationAiswarya ThomasNoch keine Bewertungen
- Incorrects On NBME ObgynDokument4 SeitenIncorrects On NBME Obgynkabal321Noch keine Bewertungen
- Exam Sample:: B. Cervical Incompetence and Cervical StenosisDokument3 SeitenExam Sample:: B. Cervical Incompetence and Cervical StenosisSiraj Ul IslamNoch keine Bewertungen
- Case 1Dokument51 SeitenCase 1Zaid ZayedNoch keine Bewertungen
- Tutor: Prof. Dr. H. Syakroni Daud Rusdi, SP - OGDokument53 SeitenTutor: Prof. Dr. H. Syakroni Daud Rusdi, SP - OGAna Abadi Al IndNoch keine Bewertungen
- Unas Mei 2020 (Sule) : Yang Dianggap Soal BaruDokument15 SeitenUnas Mei 2020 (Sule) : Yang Dianggap Soal Baruhari ilman toniNoch keine Bewertungen
- Gynaecology Case 1Dokument3 SeitenGynaecology Case 1Ivy DanNoch keine Bewertungen
- The Test May Be Run On Patients Between 22 and 34 Weeks GestationDokument6 SeitenThe Test May Be Run On Patients Between 22 and 34 Weeks Gestationdaniel_alexander_susenoNoch keine Bewertungen
- Obstetric History:: Physical ExaminationDokument2 SeitenObstetric History:: Physical ExaminationOliver Cortes AcobaNoch keine Bewertungen
- Morning Report CF + UTIDokument35 SeitenMorning Report CF + UTIdr.ronak1996Noch keine Bewertungen
- Agustus 2020Dokument24 SeitenAgustus 2020Chynthea ParamithaNoch keine Bewertungen
- Tes 1Dokument6 SeitenTes 1dika putrayudaNoch keine Bewertungen
- 2020 ANW CasesDokument7 Seiten2020 ANW CasesIvy DanNoch keine Bewertungen
- Juli 2022Dokument28 SeitenJuli 2022Chynthea ParamithaNoch keine Bewertungen
- Form 6Dokument20 SeitenForm 6walt65Noch keine Bewertungen
- Extra CasesDokument1 SeiteExtra CasesE.J. PelayoNoch keine Bewertungen
- Soal Latihan Ugm Oktober 2023Dokument28 SeitenSoal Latihan Ugm Oktober 2023Anonymous mXLu20jNoch keine Bewertungen
- DR Nadine Rev All (Samra's Edition)Dokument313 SeitenDR Nadine Rev All (Samra's Edition)Cyril I.Makar100% (1)
- Prometric Mcqs For General Practitioner GP Doctor Mcqs Exam QuestionsDokument28 SeitenPrometric Mcqs For General Practitioner GP Doctor Mcqs Exam QuestionsDr. Saqib RazaNoch keine Bewertungen
- Obstetrics Patient M.L. 26/F Date Admitted: December 17, 2018 Date Discharged: December 19, 2018 Informant: Patient Reliability: 80%Dokument6 SeitenObstetrics Patient M.L. 26/F Date Admitted: December 17, 2018 Date Discharged: December 19, 2018 Informant: Patient Reliability: 80%Justin LamNoch keine Bewertungen
- Ats Menjawab Soal Unas November 2021 EditedDokument26 SeitenAts Menjawab Soal Unas November 2021 Editedanton suponoNoch keine Bewertungen
- Final Exam Flash Cards - PDokument37 SeitenFinal Exam Flash Cards - PReut shapiraNoch keine Bewertungen
- Obg - Case Presentation - FGRDokument24 SeitenObg - Case Presentation - FGRNazee NazreenNoch keine Bewertungen
- UNAS 59th (NOV 2020) FIXDokument23 SeitenUNAS 59th (NOV 2020) FIXmhariskurniawanNoch keine Bewertungen
- Obs 1 Bleeding in Early Pregnancy QuestionsDokument9 SeitenObs 1 Bleeding in Early Pregnancy QuestionsSalmonella TyphiNoch keine Bewertungen
- Soal Ujian R2 FixedDokument9 SeitenSoal Ujian R2 Fixedprakoso jatiNoch keine Bewertungen
- PP Type Ii AnteriorDokument10 SeitenPP Type Ii AnteriorAiman ArifinNoch keine Bewertungen
- Block 1Dokument25 SeitenBlock 1Mohammad MansourNoch keine Bewertungen
- Presentation Breast Lump 1Dokument24 SeitenPresentation Breast Lump 1Khalid RizwanNoch keine Bewertungen
- CWU Gynae Missed MiscarriageDokument8 SeitenCWU Gynae Missed MiscarriageFaris Mohd NasirNoch keine Bewertungen
- TUTORIALDokument49 SeitenTUTORIALAna Abadi Al IndNoch keine Bewertungen
- Obstetrics N Gynaecology MADE EASYDokument7 SeitenObstetrics N Gynaecology MADE EASYGM SiriNoch keine Bewertungen
- Clinical-Management STRATOG NEWDokument8 SeitenClinical-Management STRATOG NEWFarrukh Ali Khan100% (1)
- Soal Usulan UnHas Juli 2019Dokument25 SeitenSoal Usulan UnHas Juli 2019Ibnu SinaNoch keine Bewertungen
- USULDokument6 SeitenUSULdika putrayudaNoch keine Bewertungen
- Myomectomy and Emergency Lap.Dokument19 SeitenMyomectomy and Emergency Lap.SirAdjeteyNoch keine Bewertungen
- Krok 2 2002 2003 Obs and GynDokument16 SeitenKrok 2 2002 2003 Obs and GynNishat_Fatima_3779Noch keine Bewertungen
- Step 2 CK - NBME 7 Answers UncompleteDokument16 SeitenStep 2 CK - NBME 7 Answers UncompleteDuke83% (12)
- Ats Menjawab Super Brankas Soal Unas 2020-2015Dokument424 SeitenAts Menjawab Super Brankas Soal Unas 2020-2015anton suponoNoch keine Bewertungen
- Ong Cases Final-1Dokument49 SeitenOng Cases Final-1Cedric KyekyeNoch keine Bewertungen
- Gynecology 2020 Copy 2Dokument620 SeitenGynecology 2020 Copy 2school adressNoch keine Bewertungen
- MCQ 22 PDFDokument7 SeitenMCQ 22 PDFirynNoch keine Bewertungen
- Obstetrics and Gynaecology Write Up 3Dokument10 SeitenObstetrics and Gynaecology Write Up 3Luqman HarunNoch keine Bewertungen
- Specimen Case Presentation Write-Up Obstetrics Case SummaryDokument9 SeitenSpecimen Case Presentation Write-Up Obstetrics Case SummaryAngeline RodriguesNoch keine Bewertungen
- Step 2 Cs ClosureDokument12 SeitenStep 2 Cs Closurewalt65100% (1)
- Rembenber Behaviorscience - OdtDokument4 SeitenRembenber Behaviorscience - Odtwalt65Noch keine Bewertungen
- Structure and Function of The Endocrine SystemDokument53 SeitenStructure and Function of The Endocrine Systemwalt65Noch keine Bewertungen
- History Taking PDFDokument12 SeitenHistory Taking PDFChenthanKrishNoch keine Bewertungen
- Remenberphama OdtDokument14 SeitenRemenberphama Odtwalt65Noch keine Bewertungen
- Review Step 2Dokument5 SeitenReview Step 2walt65Noch keine Bewertungen
- Remenberstep2 OdtDokument5 SeitenRemenberstep2 Odtwalt65Noch keine Bewertungen
- Rembenber Behaviorscience - OdtDokument4 SeitenRembenber Behaviorscience - Odtwalt65Noch keine Bewertungen
- Ckform 7Dokument21 SeitenCkform 7walt65100% (1)
- Cms Psych 3.odtDokument19 SeitenCms Psych 3.odtwalt65Noch keine Bewertungen
- Cms Psych 3.odtDokument19 SeitenCms Psych 3.odtwalt65Noch keine Bewertungen
- Cms Psych 3.odtDokument19 SeitenCms Psych 3.odtwalt65Noch keine Bewertungen
- 2014 Step 2 CK Recommended Course Order PDFDokument6 Seiten2014 Step 2 CK Recommended Course Order PDFwalt65Noch keine Bewertungen
- Form 6Dokument20 SeitenForm 6walt65Noch keine Bewertungen
- NeurologyDokument44 SeitenNeurologywalt65Noch keine Bewertungen
- RenalDokument49 SeitenRenalwalt65Noch keine Bewertungen
- Immunology ReviewDokument53 SeitenImmunology Reviewwalt65Noch keine Bewertungen
- HalleluYaH Scriptures - Book of MattithYaHuDokument39 SeitenHalleluYaH Scriptures - Book of MattithYaHuscribduser2016Noch keine Bewertungen
- Heavy Periods 6 Pads/day: CasesDokument31 SeitenHeavy Periods 6 Pads/day: Caseswalt65Noch keine Bewertungen
- PharmacoDokument33 SeitenPharmacowalt65Noch keine Bewertungen
- Renal Organ SystemDokument161 SeitenRenal Organ Systemwalt65Noch keine Bewertungen
- Lippin Cort Soft Notes RenalDokument3 SeitenLippin Cort Soft Notes Renalwalt65Noch keine Bewertungen
- Lippin NotesDokument8 SeitenLippin Noteswalt65100% (1)
- Step2 Cs DDX and SymptomsDokument8 SeitenStep2 Cs DDX and Symptomswalt65Noch keine Bewertungen
- Anatomy MiscDokument4 SeitenAnatomy MiscZachary ReiffNoch keine Bewertungen
- RenalDokument10 SeitenRenalHarris RomanosNoch keine Bewertungen
- Step 1 Topics For CKDokument5 SeitenStep 1 Topics For CKwalt65Noch keine Bewertungen
- Embryo MnemonicsDokument4 SeitenEmbryo MnemonicsJoel WarshNoch keine Bewertungen
- GeneticsDokument4 SeitenGeneticsEliza SparkNoch keine Bewertungen
- CXC - Past - Paper - 2022 Solutions PDFDokument17 SeitenCXC - Past - Paper - 2022 Solutions PDFDarren Fraser100% (1)
- Behavior Specific Praise Statements HandoutDokument3 SeitenBehavior Specific Praise Statements HandoutDaniel BernalNoch keine Bewertungen
- Intershield803 MDSDokument4 SeitenIntershield803 MDSSahanNoch keine Bewertungen
- Task 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Dokument5 SeitenTask 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Samir Mosquera-PalominoNoch keine Bewertungen
- Study Notes On Isomers and Alkyl HalidesDokument3 SeitenStudy Notes On Isomers and Alkyl HalidesChristian Josef AvelinoNoch keine Bewertungen
- Comprehensive Safe Hospital FrameworkDokument12 SeitenComprehensive Safe Hospital FrameworkEbby OktaviaNoch keine Bewertungen
- Dri InternshipDokument38 SeitenDri InternshipGuruprasad Sanga100% (3)
- 10 2005 Dec QDokument6 Seiten10 2005 Dec Qspinster40% (1)
- Covid-19 Mitigation PlanDokument8 SeitenCovid-19 Mitigation PlanEkum EdunghuNoch keine Bewertungen
- Sav4747 PDFDokument49 SeitenSav4747 PDFAndres Antonio Moreno CastroNoch keine Bewertungen
- Money Tree International Finance Corp. Checklist of Standard Loan RequirementsDokument2 SeitenMoney Tree International Finance Corp. Checklist of Standard Loan RequirementsAgape LabuntogNoch keine Bewertungen
- BMJ 40 13Dokument8 SeitenBMJ 40 13Alvin JiwonoNoch keine Bewertungen
- Analysis of Pure Copper - A Comparison of Analytical MethodsDokument12 SeitenAnalysis of Pure Copper - A Comparison of Analytical Methodsban bekasNoch keine Bewertungen
- Standards Spec Brochure ME WEBDokument44 SeitenStandards Spec Brochure ME WEBReza TambaNoch keine Bewertungen
- Jun Judging ClinicDokument1 SeiteJun Judging Cliniccsponseller27Noch keine Bewertungen
- Doctors ListDokument212 SeitenDoctors ListSaranya Chandrasekar33% (3)
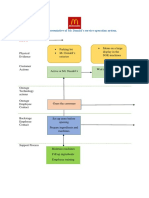
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDokument2 SeitenBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNoch keine Bewertungen
- IsoTherming® Hydroprocessing TechnologyDokument4 SeitenIsoTherming® Hydroprocessing Technologyromi moriNoch keine Bewertungen
- Ras Shastra PPT 6Dokument10 SeitenRas Shastra PPT 6Soham BhureNoch keine Bewertungen
- Compartment SyndromeDokument14 SeitenCompartment SyndromedokteraanNoch keine Bewertungen
- ASOTDokument4 SeitenASOTemperors_nestNoch keine Bewertungen
- Pigeon Disease - The Eight Most Common Health Problems in PigeonsDokument2 SeitenPigeon Disease - The Eight Most Common Health Problems in Pigeonscc_lawrence100% (1)
- EV Hammer Impact Crusher - ENDokument8 SeitenEV Hammer Impact Crusher - ENKeshav NandaNoch keine Bewertungen
- Inverter 1 KW ManualDokument44 SeitenInverter 1 KW ManualLeonardoNoch keine Bewertungen
- ZX110to330 ELEC E PDFDokument1 SeiteZX110to330 ELEC E PDFYadi100% (1)
- Fill The Gaps With The Correct WordsDokument2 SeitenFill The Gaps With The Correct WordsAlayza ChangNoch keine Bewertungen
- Impact of Employee Motivation in The Banking SectorDokument48 SeitenImpact of Employee Motivation in The Banking Sectormohd talalNoch keine Bewertungen
- Itrogen: by Deborah A. KramerDokument18 SeitenItrogen: by Deborah A. KramernycNoch keine Bewertungen
- Rooftop Rain Water Harvesting in An Educational CampusDokument9 SeitenRooftop Rain Water Harvesting in An Educational CampusAkshay BoratiNoch keine Bewertungen
- DX340LC: Crawler ExcavatorDokument20 SeitenDX340LC: Crawler ExcavatorFeristha Meriani TabitaNoch keine Bewertungen
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarVon EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarBewertung: 5 von 5 Sternen5/5 (351)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 4.5 von 5 Sternen4.5/5 (3)
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessVon EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessNoch keine Bewertungen
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- Summary of Mary Claire Haver's The Galveston DietVon EverandSummary of Mary Claire Haver's The Galveston DietBewertung: 5 von 5 Sternen5/5 (1)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeVon EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeBewertung: 4 von 5 Sternen4/5 (3)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyVon EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNoch keine Bewertungen
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthVon EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthBewertung: 4 von 5 Sternen4/5 (6)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (378)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeVon EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeBewertung: 4 von 5 Sternen4/5 (3)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodVon EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNoch keine Bewertungen
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomVon EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomBewertung: 4 von 5 Sternen4/5 (1)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsVon EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsBewertung: 4 von 5 Sternen4/5 (49)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainVon EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainBewertung: 3.5 von 5 Sternen3.5/5 (38)
- Molecules of Emotion: Why You Feel the Way You FeelVon EverandMolecules of Emotion: Why You Feel the Way You FeelBewertung: 4 von 5 Sternen4/5 (128)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingVon EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingBewertung: 4 von 5 Sternen4/5 (3)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouVon EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNoch keine Bewertungen
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthVon EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNoch keine Bewertungen
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesVon EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesNoch keine Bewertungen
- The End of Craving: Recovering the Lost Wisdom of Eating WellVon EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellBewertung: 4.5 von 5 Sternen4.5/5 (81)
- Keto Friendly Recipes: Easy Keto For Busy PeopleVon EverandKeto Friendly Recipes: Easy Keto For Busy PeopleBewertung: 3.5 von 5 Sternen3.5/5 (2)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeVon EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeBewertung: 5 von 5 Sternen5/5 (1)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseVon EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseBewertung: 4.5 von 5 Sternen4.5/5 (84)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingVon EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingBewertung: 5 von 5 Sternen5/5 (61)