Das könnte Ihnen auch gefallen
- Micro-Para Answer Key-PINK PACOPDokument31 SeitenMicro-Para Answer Key-PINK PACOPArk Olfato ParojinogNoch keine Bewertungen
- W.H.O. Murdered Africa by Dr. William Campbell DouglasDokument20 SeitenW.H.O. Murdered Africa by Dr. William Campbell DouglasJohn Burns100% (4)
- Medical Evaluation Form 2022Dokument2 SeitenMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- Early Hepatitis B Vaccines and The Man-Made Origin of HIV-AIDSDokument19 SeitenEarly Hepatitis B Vaccines and The Man-Made Origin of HIV-AIDSsupertech86Noch keine Bewertungen
- PSM Park MCQsDokument91 SeitenPSM Park MCQsGIST (Gujarat Institute of Science & Technology)82% (28)
- Medical Exam Report FormDokument4 SeitenMedical Exam Report FormSOU FEI Ang0% (1)
- Lesson8 Pediatric Health HistoryDokument9 SeitenLesson8 Pediatric Health HistoryDennis Nabor Muñoz, RN,RM100% (1)
- DHS CFS 600 Certificate of Child Examination Form IL444-4737Dokument2 SeitenDHS CFS 600 Certificate of Child Examination Form IL444-4737ArtueroNoch keine Bewertungen
- Pre-Existing Medical Conditions FormDokument3 SeitenPre-Existing Medical Conditions Formraysa mendezNoch keine Bewertungen
- Minor Life QDokument1 SeiteMinor Life QSharath_Chandh_5634Noch keine Bewertungen
- Student Medical RecordDokument3 SeitenStudent Medical Recordhamsa RasbiehNoch keine Bewertungen
- Physician S Health Evaluation FormDokument2 SeitenPhysician S Health Evaluation FormJessica Mayleen MartinezNoch keine Bewertungen
- Physician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Dokument4 SeitenPhysician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Arturo MBNoch keine Bewertungen
- Au Pair Medical RecordDokument2 SeitenAu Pair Medical RecordSamir Antonio Garcia BarrancoNoch keine Bewertungen
- OGUK Medical FormDokument7 SeitenOGUK Medical Formum erNoch keine Bewertungen
- Please Complete in Full or Attach A Copy of Your Child's Vaccination Record To The FormDokument2 SeitenPlease Complete in Full or Attach A Copy of Your Child's Vaccination Record To The FormRohit JNoch keine Bewertungen
- Medical and Physical Exam FormDokument2 SeitenMedical and Physical Exam FormkhohannahfaithNoch keine Bewertungen
- Brendahs Medical FormDokument2 SeitenBrendahs Medical FormBaluku GeofreyNoch keine Bewertungen
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Dokument6 SeitenPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieNoch keine Bewertungen
- Physician S Report FormDokument4 SeitenPhysician S Report FormpaolaNoch keine Bewertungen
- AFS Application Health FormDokument2 SeitenAFS Application Health FormPedro KunstNoch keine Bewertungen
- Paediatric HistoryDokument7 SeitenPaediatric HistoryJess WesternNoch keine Bewertungen
- Personal Health History: Complete Incomplete Don't Know Females Only LMP (Last Menstrual Period)Dokument3 SeitenPersonal Health History: Complete Incomplete Don't Know Females Only LMP (Last Menstrual Period)ERICKA GRACE DA SILVANoch keine Bewertungen
- NEW PE FORM Bangayan Vhynee SDokument4 SeitenNEW PE FORM Bangayan Vhynee SVhynee BangayanNoch keine Bewertungen
- Health Declaration FormDokument3 SeitenHealth Declaration FormMaja Aira BumatayNoch keine Bewertungen
- Texas Department of State Health Services Tuberculosis Health Assessment/HistoryDokument2 SeitenTexas Department of State Health Services Tuberculosis Health Assessment/HistoryMohd Faiz Mohd ZinNoch keine Bewertungen
- Health History Form: Personal Information - Applicant Complete This SectionDokument2 SeitenHealth History Form: Personal Information - Applicant Complete This SectionFilip MeđimorecNoch keine Bewertungen
- Medical FormDokument2 SeitenMedical FormHoney AliNoch keine Bewertungen
- Medical History FormDokument3 SeitenMedical History FormJalisha SarmientoNoch keine Bewertungen
- Au Pair Health CertificateDokument4 SeitenAu Pair Health CertificateLara KrollNoch keine Bewertungen
- Health Form A2Dokument2 SeitenHealth Form A2Dane MagruderNoch keine Bewertungen
- Student Health Services Form 2020Dokument2 SeitenStudent Health Services Form 2020Asiaui HendersonNoch keine Bewertungen
- Medical history formDokument6 SeitenMedical history formYasmin SawyerNoch keine Bewertungen
- Flu Consent FormDokument2 SeitenFlu Consent FormTiger Palm TigerNoch keine Bewertungen
- 4 PaDokument4 Seiten4 PaGermin CesaNoch keine Bewertungen
- Consent Form 2020 - Filled PDFDokument1 SeiteConsent Form 2020 - Filled PDFsudhir12345Noch keine Bewertungen
- LLC Health FormDokument2 SeitenLLC Health Formcesar maguigadNoch keine Bewertungen
- Year 9 Camp Health and Medical ConsentDokument3 SeitenYear 9 Camp Health and Medical ConsentFiona CharringtonNoch keine Bewertungen
- CT Health RecordDokument3 SeitenCT Health RecordChettamilsNoch keine Bewertungen
- School District Health Assessment FormDokument2 SeitenSchool District Health Assessment FormAnuvratha NarayananNoch keine Bewertungen
- Activity 2 (Big Leaps)Dokument4 SeitenActivity 2 (Big Leaps)Cameron De GuzmanNoch keine Bewertungen
- Medical Declaration Form: Family History of The ApplicantDokument3 SeitenMedical Declaration Form: Family History of The ApplicantJae WaiNoch keine Bewertungen
- LTP On Student Medical Records - Apsa Circular 8 SignedDokument3 SeitenLTP On Student Medical Records - Apsa Circular 8 SignedrorororNoch keine Bewertungen
- Healing Spa Intake FormsDokument9 SeitenHealing Spa Intake FormsNaura CorporationNoch keine Bewertungen
- Medical Application Form ReviewDokument3 SeitenMedical Application Form ReviewDidier G PeñuelaNoch keine Bewertungen
- Ob History Form PDFDokument2 SeitenOb History Form PDFRoan Marie JumaquioNoch keine Bewertungen
- Page 3 6 MHR PRESCREEN QUESTIONNAIREDokument5 SeitenPage 3 6 MHR PRESCREEN QUESTIONNAIREMark Joel AguilaNoch keine Bewertungen
- Medical Health Record 2 LONGDokument2 SeitenMedical Health Record 2 LONGipanagclaire8Noch keine Bewertungen
- New Employee Medical QuestionnaireDokument2 SeitenNew Employee Medical QuestionnaireRichard R M ThodéNoch keine Bewertungen
- Florida School Entry Health ExamDokument2 SeitenFlorida School Entry Health ExamPeterBurkeNoch keine Bewertungen
- Health CertificateDokument2 SeitenHealth CertificateChristos YiangouNoch keine Bewertungen
- Suspected Adverse Reaction FormDokument2 SeitenSuspected Adverse Reaction FormJonathan Deguzman100% (1)
- Libro ComplementarioDokument155 SeitenLibro ComplementarioKowe xDNoch keine Bewertungen
- Pre Medical Evaluatiom Form PFT 1 PDFDokument2 SeitenPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (1)
- 3 Health PDFDokument2 Seiten3 Health PDFpierlisurNoch keine Bewertungen
- Trek Medical FormDokument1 SeiteTrek Medical FormrenokadventuresNoch keine Bewertungen
- Olive International School Student Medical FormDokument4 SeitenOlive International School Student Medical Formlinga2014Noch keine Bewertungen
- Pediatric Health Assessment FormDokument3 SeitenPediatric Health Assessment FormCabaddu AngieNoch keine Bewertungen
- WWW - Csc.gov - PH: Additional RequirementsDokument4 SeitenWWW - Csc.gov - PH: Additional RequirementsMaria JessaNoch keine Bewertungen
- Medical Conditions Declaration Form1Dokument1 SeiteMedical Conditions Declaration Form1Khôi Mạc NguyênNoch keine Bewertungen
- Health Questionnaire: Name (Please Print)Dokument1 SeiteHealth Questionnaire: Name (Please Print)CarlosSchlozJuniorNoch keine Bewertungen
- Health Booklet 2014Dokument68 SeitenHealth Booklet 2014QwesxzNoch keine Bewertungen
- Infectious Diseases in Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandInfectious Diseases in Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementVon EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNoch keine Bewertungen
- RegistrationDokument1 SeiteRegistrationapi-247134277Noch keine Bewertungen
- Ebsa Wildkits Softball DayDokument1 SeiteEbsa Wildkits Softball Dayapi-247134277Noch keine Bewertungen
- 2018 Varsity ScheduleDokument1 Seite2018 Varsity Scheduleapi-247134277Noch keine Bewertungen
- 12 5 17 Informational MeetingDokument2 Seiten12 5 17 Informational Meetingapi-247134277Noch keine Bewertungen
- Important Monthly Current Affairs Capsule - October 2022Dokument382 SeitenImportant Monthly Current Affairs Capsule - October 2022FebzNoch keine Bewertungen
- Balanced Scorecard Slide 1: Divisional Task ForceDokument18 SeitenBalanced Scorecard Slide 1: Divisional Task ForceWaseem MushtaqNoch keine Bewertungen
- EPI ManualDokument73 SeitenEPI ManualRich Arocena100% (1)
- Polio PDFDokument14 SeitenPolio PDFInomy Claudia Katherine Imbiri50% (2)
- Section 12 A Systematic Review On The Factors Affecting COVID 19 Vaccine Hesitancy in The Philippines - CommentsDokument21 SeitenSection 12 A Systematic Review On The Factors Affecting COVID 19 Vaccine Hesitancy in The Philippines - CommentsFaye AlmiraNoch keine Bewertungen
- DOHS ReportDokument489 SeitenDOHS ReportDivya TiwariNoch keine Bewertungen
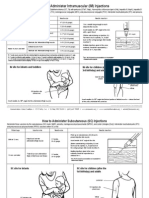
- I/M Injection Sites Acording To AgeDokument2 SeitenI/M Injection Sites Acording To Ageman0billiNoch keine Bewertungen
- Health Requirements and Recommendations For Travelers To Saudi Arabia For Hajj - 1444h (2023)Dokument9 SeitenHealth Requirements and Recommendations For Travelers To Saudi Arabia For Hajj - 1444h (2023)Latief 1711Noch keine Bewertungen
- Exam Quest Special 2023Dokument24 SeitenExam Quest Special 2023Yalvant YadavNoch keine Bewertungen
- Hajj Health Requirements English LanguageDokument8 SeitenHajj Health Requirements English Languageelis suryaniNoch keine Bewertungen
- Agenda 246th Registration BoardDokument376 SeitenAgenda 246th Registration BoardSarfarazpk1100% (2)
- Content: Trainer's Notes: ReadingDokument32 SeitenContent: Trainer's Notes: ReadingzzaentzNoch keine Bewertungen
- 1000 Doctors (And Many More) Against VivisectionDokument44 Seiten1000 Doctors (And Many More) Against VivisectionAdrian RoscowNoch keine Bewertungen
- The Truth About Polio VaccineDokument23 SeitenThe Truth About Polio Vaccinemagnumquest67% (3)
- Holding Company for Biological Products & VaccinesDokument65 SeitenHolding Company for Biological Products & Vaccineskoky123456789Noch keine Bewertungen
- SCIENTISTSDokument5 SeitenSCIENTISTSMarica Mae PreNoch keine Bewertungen
- Department of Health Programs Related To Family HealthDokument62 SeitenDepartment of Health Programs Related To Family HealthBea Bianca CruzNoch keine Bewertungen
- Eng - PB 2016 FinalDokument6 SeitenEng - PB 2016 Finalashok PradhanNoch keine Bewertungen
- Ensuring Polio Eradication in the PhilippinesDokument10 SeitenEnsuring Polio Eradication in the PhilippinesJohn Edward EscoteNoch keine Bewertungen
- Quiz On ImmunizationDokument56 SeitenQuiz On ImmunizationFreniNoch keine Bewertungen
- NCM 107A Pedia Week 8-9 Care of An InfantDokument26 SeitenNCM 107A Pedia Week 8-9 Care of An InfantInsatiable CleeNoch keine Bewertungen
- Malaysia School ImmunizationDokument41 SeitenMalaysia School ImmunizationKalai ArikaranNoch keine Bewertungen
- Poliomyelitis: The Immunological Basis For Immunization SeriesDokument32 SeitenPoliomyelitis: The Immunological Basis For Immunization SeriesTry AnitaNoch keine Bewertungen
- MCQ ImportantDokument3 SeitenMCQ ImportantSrinivas RayuduNoch keine Bewertungen
- FDA Meeting. Human Tumors For Vaccine ManufactureDokument80 SeitenFDA Meeting. Human Tumors For Vaccine ManufactureDustin Estes87% (30)
- Expanded Program On Immunization CHNDokument4 SeitenExpanded Program On Immunization CHNgeralynroseNoch keine Bewertungen