Das könnte Ihnen auch gefallen
- 2 Myasthenia Gravis and MS 2Dokument50 Seiten2 Myasthenia Gravis and MS 2Rawbeena RamtelNoch keine Bewertungen
- Myasthenia GravisDokument5 SeitenMyasthenia GravisBj DuquesaNoch keine Bewertungen
- Myasthenia GravisDokument11 SeitenMyasthenia GravisSandeepSethiNoch keine Bewertungen
- Myasthenia GravisDokument4 SeitenMyasthenia GravisArlyn MillanesNoch keine Bewertungen
- Myasthenia Gravis: Submitted ToDokument6 SeitenMyasthenia Gravis: Submitted ToRomans 6:23Noch keine Bewertungen
- Anaesthesia and Myasthenia GravisDokument12 SeitenAnaesthesia and Myasthenia Gravis37435rlcNoch keine Bewertungen
- Autoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityDokument16 SeitenAutoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityGiuseppeNoch keine Bewertungen
- Myasthenia Gravis in The Elderly: NeurologyDokument4 SeitenMyasthenia Gravis in The Elderly: NeurologyAirin QueNoch keine Bewertungen
- PharmaDokument9 SeitenPharmaمحسن حدوان عليخانNoch keine Bewertungen
- Neuromuscular Junction DisordersDokument32 SeitenNeuromuscular Junction Disordersepic sound everNoch keine Bewertungen
- Diagnosis and Management of Myasthenia Gravis: ReviewDokument9 SeitenDiagnosis and Management of Myasthenia Gravis: ReviewnetifarhatiiNoch keine Bewertungen
- Myasthenia GravisDokument31 SeitenMyasthenia Gravisjsampsonemtp100% (2)
- Myasthenia Gravis: BY Dr. S.O ItodoDokument39 SeitenMyasthenia Gravis: BY Dr. S.O ItodoIgbashioNoch keine Bewertungen
- Motor Endplate Disorders Myasthenia Gravis Overview and DefinitionDokument4 SeitenMotor Endplate Disorders Myasthenia Gravis Overview and DefinitionPJHGNoch keine Bewertungen
- EBNDokument22 SeitenEBNLouis Ann BautistaNoch keine Bewertungen
- Myasthenic Crisis As A Side Effect of Methimazole Therapy: Case ReportDokument5 SeitenMyasthenic Crisis As A Side Effect of Methimazole Therapy: Case ReportThein Htun NaungNoch keine Bewertungen
- Per A Gallo 2017Dokument6 SeitenPer A Gallo 2017Lissaberti AmaliahNoch keine Bewertungen
- Myasthenia Gravis: BY Dr. S.O ItodoDokument39 SeitenMyasthenia Gravis: BY Dr. S.O Itodosongo sorshimaNoch keine Bewertungen
- Transversemyelitis: Shin C. Beh,, Benjamin M. Greenberg,, Teresa Frohman,, Elliot M. FrohmanDokument60 SeitenTransversemyelitis: Shin C. Beh,, Benjamin M. Greenberg,, Teresa Frohman,, Elliot M. FrohmanRoxana CioflîncNoch keine Bewertungen
- Autoimmune Processes: Dr. Lubna DwerijDokument46 SeitenAutoimmune Processes: Dr. Lubna DwerijNoor MajaliNoch keine Bewertungen
- Myasthenia Gravis (2016-2017) Lecture NotesDokument9 SeitenMyasthenia Gravis (2016-2017) Lecture NotesJibril AbdulMumin KamfalaNoch keine Bewertungen
- Autoimmune 001Dokument5 SeitenAutoimmune 001Chidera Henry MaduekeNoch keine Bewertungen
- Bja MGDokument6 SeitenBja MGVignesh VenkatesanNoch keine Bewertungen
- Pediatric Myasthenia Gravis: PathophysiologyDokument6 SeitenPediatric Myasthenia Gravis: PathophysiologyLissaberti AmaliahNoch keine Bewertungen
- Uk MSDokument6 SeitenUk MScode212Noch keine Bewertungen
- Multiple SklerosisDokument16 SeitenMultiple SklerosisWisnu Lisa PratiwiNoch keine Bewertungen
- Disorders of The Neuromuscular Junction: Myasthenia GravisDokument7 SeitenDisorders of The Neuromuscular Junction: Myasthenia GravisZain AlAbideen AlTaeeNoch keine Bewertungen
- 114 Clinical Evaluation and Management of Myasthenia Gravis - DONEDokument22 Seiten114 Clinical Evaluation and Management of Myasthenia Gravis - DONEpyshcotNoch keine Bewertungen
- Transverse MyelitisDokument7 SeitenTransverse MyelitisAmr BashaNoch keine Bewertungen
- Optimizing Therapeutics in The Management of Patients With Multiple Sclerosis: A Review of Drug Efficacy, Dosing, and Mechanisms of ActionDokument12 SeitenOptimizing Therapeutics in The Management of Patients With Multiple Sclerosis: A Review of Drug Efficacy, Dosing, and Mechanisms of ActionAndhita Satya Pratama GiovanniNoch keine Bewertungen
- Multiple Slerosis: Presented by HARSHA.JDokument43 SeitenMultiple Slerosis: Presented by HARSHA.JAgatha SharmaNoch keine Bewertungen
- Multiple Sclerosis: Neurovascular DisordersDokument18 SeitenMultiple Sclerosis: Neurovascular DisordersNdoo NdooNoch keine Bewertungen
- Transverse Myelitis 2013Dokument60 SeitenTransverse Myelitis 2013Habib G. Moutran BarrosoNoch keine Bewertungen
- Tratament of Miastenia GravisDokument9 SeitenTratament of Miastenia GravisAndres MardonesNoch keine Bewertungen
- Sindrome Paraneoplasico Neurologico NejmDokument12 SeitenSindrome Paraneoplasico Neurologico NejmFernando Rodriguez BayonaNoch keine Bewertungen
- Myasthenia Gravis A ReviewDokument10 SeitenMyasthenia Gravis A ReviewAnonymous syRbQm6Noch keine Bewertungen
- Myasthenia Gravis: Moderator: DR Anitha PG: DR VijethaDokument45 SeitenMyasthenia Gravis: Moderator: DR Anitha PG: DR VijethaJerusha VijethaNoch keine Bewertungen
- Acute Lymphoblastic Leukemia DR - Hussein AlatabiDokument21 SeitenAcute Lymphoblastic Leukemia DR - Hussein AlatabiSaman SarKoNoch keine Bewertungen
- Case Study Myasthenia GravisDokument9 SeitenCase Study Myasthenia GravisYow Mabalot100% (1)
- Medical Progress: Rain UmorsDokument10 SeitenMedical Progress: Rain UmorsMoan JosNoch keine Bewertungen
- Myasthenia Gravis (MG) : Respiratory FailureDokument2 SeitenMyasthenia Gravis (MG) : Respiratory Failureclumsy16Noch keine Bewertungen
- Understanding Myasthenia Gravis: Causes, Symptoms, and TreatmentDokument5 SeitenUnderstanding Myasthenia Gravis: Causes, Symptoms, and TreatmentvaishnaviNoch keine Bewertungen
- Search Criteria: Table 1Dokument16 SeitenSearch Criteria: Table 1Armansyah Nur DewantaraNoch keine Bewertungen
- Myasthenia Gravis Lecture 12Dokument59 SeitenMyasthenia Gravis Lecture 12Pop D. MadalinaNoch keine Bewertungen
- Chapter 023 PharmacologyDokument5 SeitenChapter 023 PharmacologyLLLJJJNoch keine Bewertungen
- Trigeminal Neuralgia PDFDokument4 SeitenTrigeminal Neuralgia PDFCHenyLeeNoch keine Bewertungen
- Myasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaDokument9 SeitenMyasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaMasDhedotNoch keine Bewertungen
- Inflammatory Muscle Diseases NEJM 2015 Marinos DalakasDokument14 SeitenInflammatory Muscle Diseases NEJM 2015 Marinos DalakasWalther Seven VGNoch keine Bewertungen
- Myesthenia Gravis MedscapeDokument8 SeitenMyesthenia Gravis MedscapeSarah OvinithaNoch keine Bewertungen
- Department of Internal Medicine,: Prof WBP Matuja Muhas/MnhDokument31 SeitenDepartment of Internal Medicine,: Prof WBP Matuja Muhas/MnhDanyu KibuguluNoch keine Bewertungen
- Presented By: VIVEK DEVDokument38 SeitenPresented By: VIVEK DEVFranchesca LugoNoch keine Bewertungen
- JANIACSADI-Myasthenic Crisis Guidelines For Prevention and Treatment-Journal of The Neurological Sciences-2007 - 2Dokument7 SeitenJANIACSADI-Myasthenic Crisis Guidelines For Prevention and Treatment-Journal of The Neurological Sciences-2007 - 2Inbar Surya SeruNoch keine Bewertungen
- Myasthenia GravisDokument47 SeitenMyasthenia Gravismirabel IvanaliNoch keine Bewertungen
- Multiple Sclerosis, Myasthenia Gravis, GBSDokument12 SeitenMultiple Sclerosis, Myasthenia Gravis, GBSpertinenteNoch keine Bewertungen
- CME Article 2010 JulyDokument10 SeitenCME Article 2010 JulyIlda EscalanteNoch keine Bewertungen
- 1r70omiDokument6 Seiten1r70omiKartini tenNoch keine Bewertungen
- Myasthenia Gravis: Murali Thavasothy DCH MRCP FRCA Nicholas Hirsch FRCADokument3 SeitenMyasthenia Gravis: Murali Thavasothy DCH MRCP FRCA Nicholas Hirsch FRCAMirela CiobanescuNoch keine Bewertungen
- EY Ripe For Investment The Indonesian Health Care Industry Post Introduction of Universal Health CoverageDokument76 SeitenEY Ripe For Investment The Indonesian Health Care Industry Post Introduction of Universal Health CoverageIka Wulan PermataNoch keine Bewertungen
- WHO Dengue Guidelines 2013Dokument160 SeitenWHO Dengue Guidelines 2013Jason MirasolNoch keine Bewertungen
- Myasthenia GravisDokument25 SeitenMyasthenia GravisIka Wulan PermataNoch keine Bewertungen
- EY Ripe For Investment The Indonesian Health Care Industry Post Introduction of Universal Health CoverageDokument76 SeitenEY Ripe For Investment The Indonesian Health Care Industry Post Introduction of Universal Health CoverageIka Wulan PermataNoch keine Bewertungen
- JNC 8Dokument14 SeitenJNC 8amiwahyuniNoch keine Bewertungen
- Alcoholic Liver DiseaseDokument22 SeitenAlcoholic Liver DiseaseVikramjeet SinghNoch keine Bewertungen
- Pneumonia Nosokomial Pedoman Diagnosis Dan Penatalaksanaan Di IndonesiaDokument17 SeitenPneumonia Nosokomial Pedoman Diagnosis Dan Penatalaksanaan Di IndonesiaOkta Adinanto P100% (1)
- Amino Acid Sequences Reveal Evolutionary RelationshipsDokument6 SeitenAmino Acid Sequences Reveal Evolutionary RelationshipsAbby Gail DigalNoch keine Bewertungen
- Focusing Instruction ManualDokument15 SeitenFocusing Instruction Manualplan2222100% (1)
- Sri Padmavathi Medical College Hospital: APPLICATIONS Are INVITED For The Following Post - 2013-14Dokument3 SeitenSri Padmavathi Medical College Hospital: APPLICATIONS Are INVITED For The Following Post - 2013-14Birupakshya RoutNoch keine Bewertungen
- CP Angle SOLDokument8 SeitenCP Angle SOLVinay GNoch keine Bewertungen
- What Are The Types of EndosDokument3 SeitenWhat Are The Types of EndosSailu KatragaddaNoch keine Bewertungen
- Essential Ayurveda BookDokument196 SeitenEssential Ayurveda BookRoberto89% (9)
- Chapter 4Dokument7 SeitenChapter 4R LashNoch keine Bewertungen
- L.D..Occlusion in FPDDokument138 SeitenL.D..Occlusion in FPDApurva Deshmukh67% (3)
- Inguinal CanalDokument4 SeitenInguinal CanalspiraldaoNoch keine Bewertungen
- Magnetic Resonance Imaging Free Surfer SoftwareDokument86 SeitenMagnetic Resonance Imaging Free Surfer SoftwareDenise MathreNoch keine Bewertungen
- How Sleeping Positions Impact Sleep Quality and HealthDokument2 SeitenHow Sleeping Positions Impact Sleep Quality and HealthNeelesh Suteri0% (1)
- Blue Bio V DoH and HFMADokument21 SeitenBlue Bio V DoH and HFMAShane StarlingNoch keine Bewertungen
- T2DMDokument24 SeitenT2DMXyra BadangayonNoch keine Bewertungen
- Pengaruh Faktor-Faktor Psikososial Dan Insomnia Terhadap Depresi Pada Lansia Di Kota YogyakartaDokument5 SeitenPengaruh Faktor-Faktor Psikososial Dan Insomnia Terhadap Depresi Pada Lansia Di Kota YogyakartaKristina Puji LestariNoch keine Bewertungen
- 1-Aarogyam 1.2 - PO4080828012-204Dokument10 Seiten1-Aarogyam 1.2 - PO4080828012-204jannyyatinNoch keine Bewertungen
- Anatomy and Diseases of The UveaDokument102 SeitenAnatomy and Diseases of The UveaVishakh IsloorNoch keine Bewertungen
- 8 Science NCERT Solutions Chapter 10Dokument7 Seiten8 Science NCERT Solutions Chapter 10Raj Anand100% (1)
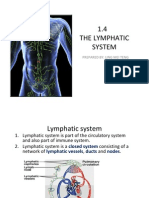
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDokument15 Seiten1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNoch keine Bewertungen
- HeparinDokument2 SeitenHeparinNinoska Garcia-Ortiz100% (4)
- ADDISONS DSE - Etio Trends&Issues + DSDokument9 SeitenADDISONS DSE - Etio Trends&Issues + DSgraceNoch keine Bewertungen
- Assessing Lateral Hip StabilityDokument7 SeitenAssessing Lateral Hip StabilityCristian Alejandro Flores PinuerNoch keine Bewertungen
- CSIR UGC JRF Subjetive Model Test PaperDokument17 SeitenCSIR UGC JRF Subjetive Model Test PaperManu Mallahalli ShanthappaNoch keine Bewertungen
- Pete Pfitzinger Advanced Marathoning Training 88K-1Dokument8 SeitenPete Pfitzinger Advanced Marathoning Training 88K-1Phan ToanNoch keine Bewertungen
- Musculoskeletal System Lecture NotesDokument169 SeitenMusculoskeletal System Lecture Noteszygote0711578796% (28)
- NCM 103 RLE NOTESDokument8 SeitenNCM 103 RLE NOTESgallardo.bettinarose.iNoch keine Bewertungen
- Arthropod-Plant Interactions Novel Insights and Approaches For IPMDokument238 SeitenArthropod-Plant Interactions Novel Insights and Approaches For IPMAnonymous T9uyM2Noch keine Bewertungen
- Biology PDFDokument1.447 SeitenBiology PDFPrincess Ethel Atillo100% (2)
- Gastro-Intestinal System Diagnostic TestsDokument11 SeitenGastro-Intestinal System Diagnostic TestsFev BanataoNoch keine Bewertungen
- COPING WITH STRESSDokument16 SeitenCOPING WITH STRESSDionisius KevinNoch keine Bewertungen
- CHAPTER SUMMARY-opiod AnalgesicDokument9 SeitenCHAPTER SUMMARY-opiod AnalgesicNuttiya WerawattanachaiNoch keine Bewertungen