Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Yogananda Scientific HealingDokument47 SeitenYogananda Scientific HealingSagar Pandya100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Basics of Fire SprinklerDokument21 SeitenBasics of Fire SprinklerLeo_1982Noch keine Bewertungen
- NORSOK M-630 Edition 6 Draft For HearingDokument146 SeitenNORSOK M-630 Edition 6 Draft For Hearingcaod1712100% (1)
- Neopuff PDFDokument4 SeitenNeopuff PDFoechimNoch keine Bewertungen
- D6228 - 10Dokument8 SeitenD6228 - 10POSSDNoch keine Bewertungen
- CholesteatomaDokument9 SeitenCholesteatomamakintosh88Noch keine Bewertungen
- Set Rec Pic 899Dokument12 SeitenSet Rec Pic 899Peter SalimNoch keine Bewertungen
- Set Rec Pic 827Dokument2 SeitenSet Rec Pic 827Peter SalimNoch keine Bewertungen
- Lampiran Vaksinasi Pegawai Rsud ArosukaDokument26 SeitenLampiran Vaksinasi Pegawai Rsud ArosukaPeter SalimNoch keine Bewertungen
- Yang 2016Dokument7 SeitenYang 2016Peter SalimNoch keine Bewertungen
- Event 1128 N ADokument1 SeiteEvent 1128 N APeter SalimNoch keine Bewertungen
- Set Rec Pic 60Dokument1 SeiteSet Rec Pic 60Peter SalimNoch keine Bewertungen
- ENT014 Throat ClearingDokument2 SeitenENT014 Throat ClearingPeter SalimNoch keine Bewertungen
- Ice Cold Carbonated Water A Therapy For Persistent Hyperawareness of Pharyngeal Mucus and Throat ClearingDokument4 SeitenIce Cold Carbonated Water A Therapy For Persistent Hyperawareness of Pharyngeal Mucus and Throat ClearingPeter SalimNoch keine Bewertungen
- Proliferating Active Cells, Lymphocyte Subsets, and Dendritic Cells in Recurrent TonsillitisDokument7 SeitenProliferating Active Cells, Lymphocyte Subsets, and Dendritic Cells in Recurrent TonsillitisPeter SalimNoch keine Bewertungen
- Filessetrec SPH Item 17105Dokument3 SeitenFilessetrec SPH Item 17105Peter SalimNoch keine Bewertungen
- Set Rec Pic 827Dokument2 SeitenSet Rec Pic 827Peter SalimNoch keine Bewertungen
- Set Rec Pic 899Dokument12 SeitenSet Rec Pic 899Peter SalimNoch keine Bewertungen
- Mastoidectomy: NO Product Description Qty Image COTTLE Metal Mallet, 18 CMDokument6 SeitenMastoidectomy: NO Product Description Qty Image COTTLE Metal Mallet, 18 CMPeter SalimNoch keine Bewertungen
- Case Open Reduction BonnyDokument21 SeitenCase Open Reduction BonnyPeter SalimNoch keine Bewertungen
- Mastoid ObliterationDokument5 SeitenMastoid ObliterationPeter SalimNoch keine Bewertungen
- CASE REPORT Laser-Assisted Treatment of SialolithiasisDokument2 SeitenCASE REPORT Laser-Assisted Treatment of SialolithiasisPeter SalimNoch keine Bewertungen
- Mastoidectomy: NO Product Description Qty Image COTTLE Metal Mallet, 18 CMDokument6 SeitenMastoidectomy: NO Product Description Qty Image COTTLE Metal Mallet, 18 CMPeter SalimNoch keine Bewertungen
- Clinical, Statistical and Chemical Study of SialolithiasisDokument6 SeitenClinical, Statistical and Chemical Study of SialolithiasisPeter SalimNoch keine Bewertungen
- Logo BatasDokument1 SeiteLogo BatasPeter SalimNoch keine Bewertungen
- How To InstallDokument1 SeiteHow To InstallSodik NurhidayatNoch keine Bewertungen
- 751 FullDokument6 Seiten751 FullKsh Kim Sohyun INoch keine Bewertungen
- Instructions !!!Dokument1 SeiteInstructions !!!iindestructibleNoch keine Bewertungen
- Department of Otorhinolaryngology Head and Neck Surgery Andalas University/Dr. M. Djamil Hospital PadangDokument1 SeiteDepartment of Otorhinolaryngology Head and Neck Surgery Andalas University/Dr. M. Djamil Hospital PadangPeter SalimNoch keine Bewertungen
- 2nd Announcement Pito Xi Makassar 1Dokument4 Seiten2nd Announcement Pito Xi Makassar 1Peter SalimNoch keine Bewertungen
- 0100 6991 RCBC 41 03 00208Dokument7 Seiten0100 6991 RCBC 41 03 00208Peter SalimNoch keine Bewertungen
- pRESENTASI TURBINATESDokument50 SeitenpRESENTASI TURBINATESPeter SalimNoch keine Bewertungen
- FESS Uncapping The EggDokument28 SeitenFESS Uncapping The EggPeter SalimNoch keine Bewertungen
- Logo BatasDokument1 SeiteLogo BatasPeter SalimNoch keine Bewertungen
- 0100 6991 RCBC 41 03 00208Dokument7 Seiten0100 6991 RCBC 41 03 00208Peter SalimNoch keine Bewertungen
- Long Term Effects of Surgically Assisted Rapid Maxillary Expansion Without Performing Osteotomy of The Pterygoid PlatesDokument4 SeitenLong Term Effects of Surgically Assisted Rapid Maxillary Expansion Without Performing Osteotomy of The Pterygoid PlatesAngélica Valenzuela AndrighiNoch keine Bewertungen
- GEC - ReviewerDokument23 SeitenGEC - ReviewerGlycel BagabagonNoch keine Bewertungen
- Sustainable Development at British Petroleum: Presented by Amardeep Kulshrestha 09BS0000172 Section-EDokument20 SeitenSustainable Development at British Petroleum: Presented by Amardeep Kulshrestha 09BS0000172 Section-EAmar KulshresthaNoch keine Bewertungen
- Present Continuous Exercises Test 1 - Positive Statements ExerciseDokument2 SeitenPresent Continuous Exercises Test 1 - Positive Statements Exerciseangel omar peraltaNoch keine Bewertungen
- Pioneer PDP 5071 5070pu Arp 3354Dokument219 SeitenPioneer PDP 5071 5070pu Arp 3354Dan Prewitt100% (1)
- High Speed DoorsDokument64 SeitenHigh Speed DoorsVadimMedooffNoch keine Bewertungen
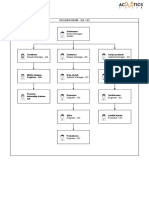
- Organogram - Qa / QC: Srinivasan SrinivasanDokument4 SeitenOrganogram - Qa / QC: Srinivasan SrinivasanGowtham VenkatNoch keine Bewertungen
- Brief RESUME EmailDokument4 SeitenBrief RESUME Emailranjit_kadalg2011Noch keine Bewertungen
- E61 DiagramDokument79 SeitenE61 Diagramthanes1027Noch keine Bewertungen
- Plica PDFDokument7 SeitenPlica PDFIVAN VERGARANoch keine Bewertungen
- Science 9 Q4 SML17 V2Dokument15 SeitenScience 9 Q4 SML17 V2HotdogNoch keine Bewertungen
- K EtaDokument14 SeitenK EtaJosue Teni BeltetonNoch keine Bewertungen
- Starkville Dispatch Eedition 9-10-20Dokument12 SeitenStarkville Dispatch Eedition 9-10-20The DispatchNoch keine Bewertungen
- G103 Remov Waste Dust Extraction UnitDokument2 SeitenG103 Remov Waste Dust Extraction UnitJoseCRomeroNoch keine Bewertungen
- TraceGains Inspection Day FDA Audit ChecklistDokument2 SeitenTraceGains Inspection Day FDA Audit Checklistdrs_mdu48Noch keine Bewertungen
- Answers To Your Questions About Circumcision and HIV/AIDSDokument2 SeitenAnswers To Your Questions About Circumcision and HIV/AIDSAlex BrownNoch keine Bewertungen
- SPA - MichaelDokument1 SeiteSPA - Michaelgilberthufana446877Noch keine Bewertungen
- Xi 3 1Dokument1 SeiteXi 3 1Krishnan KozhumamNoch keine Bewertungen
- Rules For State Competitions and Iabf Approved TournamentsDokument56 SeitenRules For State Competitions and Iabf Approved TournamentsQuality management systems documentsNoch keine Bewertungen
- Jun Judging ClinicDokument1 SeiteJun Judging Cliniccsponseller27Noch keine Bewertungen
- The Effects of Violent Video Games Research Paper English Comp2Dokument11 SeitenThe Effects of Violent Video Games Research Paper English Comp2api-451442670Noch keine Bewertungen
- Chapter Three Liquid Piping SystemDokument51 SeitenChapter Three Liquid Piping SystemMelaku TamiratNoch keine Bewertungen
- Current Concepts of Enzyme Histochemistry in Modern PathologyDokument11 SeitenCurrent Concepts of Enzyme Histochemistry in Modern PathologyRosa AquinoNoch keine Bewertungen
- Wisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseDokument3 SeitenWisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseTMJ4 NewsNoch keine Bewertungen
- Libro Resumenes 2012Dokument735 SeitenLibro Resumenes 2012fdobonat613100% (2)