Das könnte Ihnen auch gefallen
- AWWA M22 SpreadsheetDokument2 SeitenAWWA M22 SpreadsheetmassodiqNoch keine Bewertungen
- Business Report Writing SkillsDokument78 SeitenBusiness Report Writing Skillsssriram1990100% (13)
- August 2019 Atlantic Yards/Pacific Park Tech MemoDokument23 SeitenAugust 2019 Atlantic Yards/Pacific Park Tech MemoNorman OderNoch keine Bewertungen
- Referensi Product RocaDokument17 SeitenReferensi Product Rocasokogi reksaciptaNoch keine Bewertungen
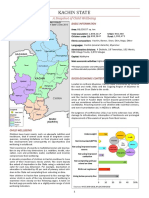
- Kachin State Profile UNICEFDokument4 SeitenKachin State Profile UNICEFmarcmyomyint1663100% (1)
- Rakhine State: A Snapshot of Child WellbeingDokument4 SeitenRakhine State: A Snapshot of Child Wellbeingmarcmyomyint1663Noch keine Bewertungen
- NalgondanggggDokument4 SeitenNalgondanggggmadara uNoch keine Bewertungen
- NutritionDokument1 SeiteNutritionUNICEF UgandaNoch keine Bewertungen
- Dietary Adequacy and Nutritional Status of Meitei CommunityDokument12 SeitenDietary Adequacy and Nutritional Status of Meitei CommunityThingnganing LongvahNoch keine Bewertungen
- POSHAN Abhiyaan PDFDokument2 SeitenPOSHAN Abhiyaan PDFVishal Pal Vishal PalNoch keine Bewertungen
- POSHAN AbhiyaanDokument2 SeitenPOSHAN AbhiyaanAnonymous x8MTGYUpNoch keine Bewertungen
- 7 +1365++harjiantiDokument10 Seiten7 +1365++harjiantiTasya RosaNoch keine Bewertungen
- Status GiziDokument7 SeitenStatus GiziaulNoch keine Bewertungen
- International Journal of MechanicalDokument8 SeitenInternational Journal of MechanicalRahma HartonoNoch keine Bewertungen
- Mid Day Meal SchemeDokument2 SeitenMid Day Meal SchemeJosine JonesNoch keine Bewertungen
- Jurnal AgnesDokument8 SeitenJurnal AgnesRosi AmeliaNoch keine Bewertungen
- HRP2015 - NUTRITION CLUSTER CHAP 2015 Inputs v2 - ICCT - 28oct2014Dokument3 SeitenHRP2015 - NUTRITION CLUSTER CHAP 2015 Inputs v2 - ICCT - 28oct2014RohullahNoch keine Bewertungen
- Republic of The Philippines Department of Education: Region V Schools Division of Sorsogon CityDokument4 SeitenRepublic of The Philippines Department of Education: Region V Schools Division of Sorsogon Cityamanda adajarNoch keine Bewertungen
- Piloting Social Protection in Chin State Myanmar Chllenges and Opportunities Within A Context of FragilityDokument6 SeitenPiloting Social Protection in Chin State Myanmar Chllenges and Opportunities Within A Context of Fragilityhpillicseng2Noch keine Bewertungen
- SSRN Id1969685Dokument19 SeitenSSRN Id1969685Muhammad AhmadNoch keine Bewertungen
- Food Security and ParentingDokument5 SeitenFood Security and ParentingraysamuslimcornerNoch keine Bewertungen
- Strengthening Peer Educator On Mother's Knowledge and Attitudes of Stunting in Ogan Komering Ilir RegencyDokument7 SeitenStrengthening Peer Educator On Mother's Knowledge and Attitudes of Stunting in Ogan Komering Ilir RegencyIts4peopleNoch keine Bewertungen
- Faktor Determinan Balita Stunting Pada DDokument14 SeitenFaktor Determinan Balita Stunting Pada DVIRGINA PUTRINoch keine Bewertungen
- Daily News Simplified - DNS Notes: SL. NO. Topics The Hindu Page NoDokument11 SeitenDaily News Simplified - DNS Notes: SL. NO. Topics The Hindu Page NoVishNoch keine Bewertungen
- Food Fortification in India: Enriching Foods, Enriching LivesDokument18 SeitenFood Fortification in India: Enriching Foods, Enriching LivesSagar SharmaNoch keine Bewertungen
- Childhood Stunting and Wasting in Myanmar Key DrivDokument8 SeitenChildhood Stunting and Wasting in Myanmar Key DrivdanskionceNoch keine Bewertungen
- Determinants of Exclusive Breastfeeding in Rural South IndiaDokument7 SeitenDeterminants of Exclusive Breastfeeding in Rural South Indiafatmawati ibrahimNoch keine Bewertungen
- Ketpang 13. Studi Kasus Ketahanan PanganDokument20 SeitenKetpang 13. Studi Kasus Ketahanan PanganDianNoch keine Bewertungen
- Why Practitioners in Development Should Integrate Nutrition: United Nations System Standing Committee On NutritionDokument43 SeitenWhy Practitioners in Development Should Integrate Nutrition: United Nations System Standing Committee On NutritionadindaNoch keine Bewertungen
- Stunting Di Desa Pilangsari Kabupaten Bojonegoro Posyandu Cadres and Mother Empowerment To Prevent Stunting Prevalence in Pilangsari Village, Bojnegoro RegencyDokument10 SeitenStunting Di Desa Pilangsari Kabupaten Bojonegoro Posyandu Cadres and Mother Empowerment To Prevent Stunting Prevalence in Pilangsari Village, Bojnegoro RegencySheni Ratna AmeliaNoch keine Bewertungen
- Ana Riandari (152221039) Tugas Penelitian Kebidanan 2 (Dosen Isfaizah, S.si.T.,MPH)Dokument12 SeitenAna Riandari (152221039) Tugas Penelitian Kebidanan 2 (Dosen Isfaizah, S.si.T.,MPH)Ana RiandariNoch keine Bewertungen
- 519 968 1 SMDokument13 Seiten519 968 1 SMRendra SyaniNoch keine Bewertungen
- Studi Kasus Ketahanan PanganDokument20 SeitenStudi Kasus Ketahanan PanganFeni AnggraeniNoch keine Bewertungen
- 149 461 1 PBDokument9 Seiten149 461 1 PBIndriani MohamadNoch keine Bewertungen
- Wipro CSR Projects 1702149035Dokument46 SeitenWipro CSR Projects 1702149035Liberal CatNoch keine Bewertungen
- Journal of StuntingDokument9 SeitenJournal of StuntingLini Anisfatus SholihahNoch keine Bewertungen
- Lnap 2023-2025 (06.07.2023)Dokument41 SeitenLnap 2023-2025 (06.07.2023)ilog ndpNoch keine Bewertungen
- Executive Summary - Pondo NG PinoyDokument9 SeitenExecutive Summary - Pondo NG PinoyFrancine de AsisNoch keine Bewertungen
- IJANS - Impact of MGNREGA To Achieve Food Security Among Rural HouseholdDokument4 SeitenIJANS - Impact of MGNREGA To Achieve Food Security Among Rural Householdiaset123Noch keine Bewertungen
- Need Assessment of Stunted Children During Pandemic Covid-19 To Develop Nutrition Intervention Program in Jember District, East Java, IndonesiaDokument6 SeitenNeed Assessment of Stunted Children During Pandemic Covid-19 To Develop Nutrition Intervention Program in Jember District, East Java, IndonesiaHumba HammuNoch keine Bewertungen
- Sociocultural Transformation in Efforts To Reduce Mortality of Infants in Bone Regency IndonesiaDokument4 SeitenSociocultural Transformation in Efforts To Reduce Mortality of Infants in Bone Regency IndonesiaidhaNoch keine Bewertungen
- 345-Article Text-1526-1-10-20210620Dokument7 Seiten345-Article Text-1526-1-10-20210620FaliyaaaNoch keine Bewertungen
- Crop Diversification-Undernutrition - CLARA JOAN JOACHIMJONES PDFDokument16 SeitenCrop Diversification-Undernutrition - CLARA JOAN JOACHIMJONES PDFClara Joan JoachimNoch keine Bewertungen
- Right To HealthDokument2 SeitenRight To HealthPiyush LabanaNoch keine Bewertungen
- 68-Article Text-402-1-10-20220930Dokument7 Seiten68-Article Text-402-1-10-20220930Ela RosyadaNoch keine Bewertungen
- Relationship of Mothers' Parenting and Stunting in Toddlers Aged 12-36 Months in Bogor Regency, West Java Province, Indonesia in 2019Dokument7 SeitenRelationship of Mothers' Parenting and Stunting in Toddlers Aged 12-36 Months in Bogor Regency, West Java Province, Indonesia in 2019Rias Pengantin Rusty MuslimahNoch keine Bewertungen
- Health Equity in MyanmarDokument5 SeitenHealth Equity in MyanmarHein Htet Aung100% (1)
- 3702 11508 1 PBDokument12 Seiten3702 11508 1 PBKHAINoch keine Bewertungen
- Assessment of Risk Factors For Severe Acute Malnutrition in Children Below The Age of FiveDokument13 SeitenAssessment of Risk Factors For Severe Acute Malnutrition in Children Below The Age of FiveKIU PUBLICATION AND EXTENSIONNoch keine Bewertungen
- National Rural Health MissionDokument39 SeitenNational Rural Health MissionDeepaNoch keine Bewertungen
- Li 2020 Oi 200162Dokument18 SeitenLi 2020 Oi 200162monojoonk94Noch keine Bewertungen
- Publication 1Dokument2 SeitenPublication 1shalom jailaNoch keine Bewertungen
- Policy Evaluation To Accelerate Stunting Prevention in Cianjur DistrictDokument6 SeitenPolicy Evaluation To Accelerate Stunting Prevention in Cianjur DistrictAJHSSR JournalNoch keine Bewertungen
- Social Protection Afghanistan briefingBTDokument7 SeitenSocial Protection Afghanistan briefingBTArun Kumar SinghNoch keine Bewertungen
- Nutrients 15 00389Dokument13 SeitenNutrients 15 00389Rofingatul MubasyirohNoch keine Bewertungen
- Jurnal StuntingDokument17 SeitenJurnal StuntingnatiyaNoch keine Bewertungen
- Jurnal Strategi Gerakan Cegah Stunting Menggunakan Metode Sosialisasi Di Desa Dara KunciDokument18 SeitenJurnal Strategi Gerakan Cegah Stunting Menggunakan Metode Sosialisasi Di Desa Dara KunciFarah Dhiyah Alfini SarnyotoNoch keine Bewertungen
- KEK Dan Berat LahirDokument13 SeitenKEK Dan Berat LahirKurnia Dwi JulianiNoch keine Bewertungen
- 1b. Children and SDGsDokument28 Seiten1b. Children and SDGsThanh MaiNoch keine Bewertungen
- 160-Article Text-1085-1-4-20220419 BaruDokument5 Seiten160-Article Text-1085-1-4-20220419 BaruNia ZahrotulNoch keine Bewertungen
- Behaviour Analaysis Powerpoint Draft - 20 Sept 2020Dokument41 SeitenBehaviour Analaysis Powerpoint Draft - 20 Sept 2020Hanina Umi SofiyanaNoch keine Bewertungen
- Sabla Proofread FormattedDokument3 SeitenSabla Proofread FormattedKeerthanaNoch keine Bewertungen
- Original Research: © 2019international Journal of Nursing and Midwiferyscience (Ijnms)Dokument11 SeitenOriginal Research: © 2019international Journal of Nursing and Midwiferyscience (Ijnms)Herkulanus ErwinNoch keine Bewertungen
- Asia and the Pacific Regional Overview of Food Security and Nutrition 2019: Placing Nutrition at the Centre of Social ProtectionVon EverandAsia and the Pacific Regional Overview of Food Security and Nutrition 2019: Placing Nutrition at the Centre of Social ProtectionNoch keine Bewertungen
- Remittance Flows From Thailand To Mawlamyine, Mon State, MyanmarDokument13 SeitenRemittance Flows From Thailand To Mawlamyine, Mon State, MyanmarThet Ko KoNoch keine Bewertungen
- Selected Media Contacts List SC - MYSAPDokument2 SeitenSelected Media Contacts List SC - MYSAPThet Ko KoNoch keine Bewertungen
- MonStateProfile June2014Dokument12 SeitenMonStateProfile June2014Thet Ko KoNoch keine Bewertungen
- 4 3 MyanmarDokument52 Seiten4 3 MyanmarThet Ko KoNoch keine Bewertungen
- Grammar For Academic Writing Ism PDFDokument94 SeitenGrammar For Academic Writing Ism PDFsarnai dandarNoch keine Bewertungen
- 2014 Burmese CensusDokument17 Seiten2014 Burmese CensusGatekeeper170Noch keine Bewertungen
- E I A Writing Style GuideDokument139 SeitenE I A Writing Style GuideThet Ko KoNoch keine Bewertungen
- Sagaing Region Profile FinalDokument4 SeitenSagaing Region Profile FinalThet Ko KoNoch keine Bewertungen
- Tat Lan Vca Report March 2014 HaDokument79 SeitenTat Lan Vca Report March 2014 HaThet Ko KoNoch keine Bewertungen
- 2001 02 GlobalizationDokument50 Seiten2001 02 GlobalizationThet Ko KoNoch keine Bewertungen
- Celebrity Politicians and Publicity Rights in The Age of ObamaDokument46 SeitenCelebrity Politicians and Publicity Rights in The Age of ObamaThet Ko KoNoch keine Bewertungen
- 2001 02 GlobalizationDokument50 Seiten2001 02 GlobalizationThet Ko KoNoch keine Bewertungen
- 50 Common English Phrasal Verbs PDFDokument54 Seiten50 Common English Phrasal Verbs PDFPapitch Do DuneNoch keine Bewertungen
- 01 Social Media PolicyDokument9 Seiten01 Social Media PolicyThet Ko KoNoch keine Bewertungen
- Ethnicity PaperDokument22 SeitenEthnicity PaperThet Ko KoNoch keine Bewertungen
- 3 Essay Bhau MikDokument20 Seiten3 Essay Bhau MikThet Ko KoNoch keine Bewertungen
- 2014 Burmese CensusDokument17 Seiten2014 Burmese CensusGatekeeper170Noch keine Bewertungen
- 2548Dokument44 Seiten2548Thet Ko KoNoch keine Bewertungen
- Celebrity Politicians and Publicity Rights in The Age of ObamaDokument46 SeitenCelebrity Politicians and Publicity Rights in The Age of ObamaThet Ko KoNoch keine Bewertungen
- Philippine Halal ActDokument7 SeitenPhilippine Halal ActThet Ko KoNoch keine Bewertungen
- Acf 2012 Myanmar Nutrition (A1y) Evaluation 2012 Full ReportDokument88 SeitenAcf 2012 Myanmar Nutrition (A1y) Evaluation 2012 Full ReportThet Ko KoNoch keine Bewertungen
- Sagaing Region Profile FinalDokument4 SeitenSagaing Region Profile FinalThet Ko KoNoch keine Bewertungen
- Endangered Holy Houses PDFDokument63 SeitenEndangered Holy Houses PDFThet Ko KoNoch keine Bewertungen
- Social Leadership CourseDokument1 SeiteSocial Leadership CourseThet Ko KoNoch keine Bewertungen
- 01 Social Media PolicyDokument9 Seiten01 Social Media PolicyThet Ko KoNoch keine Bewertungen
- European, Trade, and The Unification of Burma, C 1540-1620 by Victor B LeibermanDokument24 SeitenEuropean, Trade, and The Unification of Burma, C 1540-1620 by Victor B LeibermanThet Ko KoNoch keine Bewertungen
- Environmental Health and SanitationDokument12 SeitenEnvironmental Health and SanitationJohn WayneNoch keine Bewertungen
- Swachh Bharat Abhiyan MaharashtraDokument18 SeitenSwachh Bharat Abhiyan Maharashtra01 - Shweta BaraveNoch keine Bewertungen
- Disaster Management NotesDokument26 SeitenDisaster Management NotespecmbaNoch keine Bewertungen
- 146 PDFDokument483 Seiten146 PDFArslan SajjadNoch keine Bewertungen
- Matarba Primary School SIPDokument27 SeitenMatarba Primary School SIPHaron HB WritersNoch keine Bewertungen
- A Sample of Project Proposal by A Commun PDFDokument11 SeitenA Sample of Project Proposal by A Commun PDFIpiphaniaeFernandezItalio100% (1)
- I WR M Plan FrameworkDokument58 SeitenI WR M Plan FrameworkJovenal TuplanoNoch keine Bewertungen
- Proposed Sanitary Landfill, Okhla, New Delhi: Pre Feasibility ReportDokument32 SeitenProposed Sanitary Landfill, Okhla, New Delhi: Pre Feasibility ReportMark DeryNoch keine Bewertungen
- BHW Training EnvironmentalDokument19 SeitenBHW Training EnvironmentalWilma BeraldeNoch keine Bewertungen
- DiagramDokument12 SeitenDiagramJessica CindyNoch keine Bewertungen
- Tle9 He Beauty Care Nail Care q1 Module 6 Wilnelia P. BigayDokument12 SeitenTle9 He Beauty Care Nail Care q1 Module 6 Wilnelia P. BigayElaeca AbenNoch keine Bewertungen
- Community Health Nursing II Course SyllabusDokument14 SeitenCommunity Health Nursing II Course SyllabusJoiz Rivera100% (1)
- Daily Sanitation Inspection ChecklistDokument3 SeitenDaily Sanitation Inspection ChecklistJames Christian Hermetanio LopezNoch keine Bewertungen
- The Project For Capacity Development On Water Supply in Semi-Urban Areas in NepalDokument221 SeitenThe Project For Capacity Development On Water Supply in Semi-Urban Areas in NepalANKITNoch keine Bewertungen
- Water SanitationDokument4 SeitenWater SanitationTrina CardonaNoch keine Bewertungen
- Acww Funding Guidelines (Pre Application Information) 2017Dokument5 SeitenAcww Funding Guidelines (Pre Application Information) 2017Hunu-boafo Senyo-innocentNoch keine Bewertungen
- Gudina CVDokument5 SeitenGudina CVVo Viet AnhNoch keine Bewertungen
- Epidemiology: Open AccessDokument10 SeitenEpidemiology: Open AccessTomas Yeheis100% (1)
- Ez Roll LDokument29 SeitenEz Roll Lapi-597045564Noch keine Bewertungen
- URC - 2005 - The Case of The Teduray People in Eight Barangays of Upi, MaguindanaoDokument16 SeitenURC - 2005 - The Case of The Teduray People in Eight Barangays of Upi, MaguindanaoIP DevNoch keine Bewertungen
- Nebiyeleul Mulugeta Mersha GSE 1473.06 Research Title; the Challenges of Sewerage and Drainages Maintenance Management System in Addis Ababa City Administration the Case of Kirkos Sub City. Advisor Filmon Hadaro (Ph.D) 2017Dokument128 SeitenNebiyeleul Mulugeta Mersha GSE 1473.06 Research Title; the Challenges of Sewerage and Drainages Maintenance Management System in Addis Ababa City Administration the Case of Kirkos Sub City. Advisor Filmon Hadaro (Ph.D) 2017NebiyeleulNoch keine Bewertungen
- Brazil Law 6 360 23 September 1976 enDokument18 SeitenBrazil Law 6 360 23 September 1976 enLackner MarceloNoch keine Bewertungen
- Sewerage Conveyance SystemDokument98 SeitenSewerage Conveyance SystemVidya NaliNoch keine Bewertungen
- 10.the Inspecting Staff: A.InspectorDokument6 Seiten10.the Inspecting Staff: A.Inspectorrohan wagheNoch keine Bewertungen
- Submitted To:: Independent University, Bangladesh (Iub)Dokument28 SeitenSubmitted To:: Independent University, Bangladesh (Iub)Mashfique AhmedNoch keine Bewertungen
- Population TaguigDokument17 SeitenPopulation TaguigDerek Dylan San JoaquinNoch keine Bewertungen
- Strategic Initiative ProposalDokument32 SeitenStrategic Initiative ProposalAlie Lee GeolagaNoch keine Bewertungen