Das könnte Ihnen auch gefallen
- Inborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsVon EverandInborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsNoch keine Bewertungen
- Autoimmune Hepatitis, Overlap Syndrome, Primary Sclerosing Cholangitis and Primary Biliary Cirrhosis in Clinical PracticeVon EverandAutoimmune Hepatitis, Overlap Syndrome, Primary Sclerosing Cholangitis and Primary Biliary Cirrhosis in Clinical PracticeNoch keine Bewertungen
- Dyslipoproteinemia - Strategies for Diagnosis and TherapyVon EverandDyslipoproteinemia - Strategies for Diagnosis and TherapyNoch keine Bewertungen
- Concise Histology - Leslie P Gartner & James L Hiatt (1E)Dokument353 SeitenConcise Histology - Leslie P Gartner & James L Hiatt (1E)Subhashree Nayak94% (16)
- Endocrine Hypertension - Diagnosis and Treatment of Hormone-Induced Blood Pressure DisordersVon EverandEndocrine Hypertension - Diagnosis and Treatment of Hormone-Induced Blood Pressure DisordersNoch keine Bewertungen
- Inherited Disorders of Carbohydrate Metabolism - Glycogen Storage Diseases and Deficiencies of Monosaccharide MetabolismVon EverandInherited Disorders of Carbohydrate Metabolism - Glycogen Storage Diseases and Deficiencies of Monosaccharide MetabolismNoch keine Bewertungen
- Deficiencies of the Urea Cycle - Clinical Significance and TherapyVon EverandDeficiencies of the Urea Cycle - Clinical Significance and TherapyNoch keine Bewertungen
- Uti in WomanDokument6 SeitenUti in WomanPrimasari DiahNoch keine Bewertungen
- Spectrum and Treatment of Anaerobic InfectionsDokument13 SeitenSpectrum and Treatment of Anaerobic Infectionsluis argasNoch keine Bewertungen
- Modern Treatment of Community-Acquired Pneumonia (CAP)Von EverandModern Treatment of Community-Acquired Pneumonia (CAP)Noch keine Bewertungen
- Animal and Translational Models for CNS Drug Discovery: Neurological DisordersVon EverandAnimal and Translational Models for CNS Drug Discovery: Neurological DisordersRobert A. McArthurNoch keine Bewertungen
- Current treatment concepts for primary CNS lymphomaVon EverandCurrent treatment concepts for primary CNS lymphomaNoch keine Bewertungen
- Atlas of Endocrine Pathology - Erickson, Lori ADokument208 SeitenAtlas of Endocrine Pathology - Erickson, Lori Aoyenen100% (1)
- Murillo de Oliveira Antunes 2020Dokument15 SeitenMurillo de Oliveira Antunes 2020Asisten Lab TLPNoch keine Bewertungen
- Atlas of Spleen Pathology and Histhology CompletDokument173 SeitenAtlas of Spleen Pathology and Histhology CompletAncamed NycoletaNoch keine Bewertungen
- Animal and Translational Models for CNS Drug Discovery: Reward Deficit DisordersVon EverandAnimal and Translational Models for CNS Drug Discovery: Reward Deficit DisordersRobert A. McArthurNoch keine Bewertungen
- Inherited Disorders of Biogenic Amines: A Practical GuideVon EverandInherited Disorders of Biogenic Amines: A Practical GuideNoch keine Bewertungen
- SLE PolyautoimmunityDokument4 SeitenSLE PolyautoimmunityIsabela Rebellon MartinezNoch keine Bewertungen
- Shock – modern clinical treatment conceptsVon EverandShock – modern clinical treatment conceptsNoch keine Bewertungen
- GvHD prevention in allogeneic stem cell transplantationVon EverandGvHD prevention in allogeneic stem cell transplantationNoch keine Bewertungen
- Guia Esvs Manejo Evc 2015Dokument60 SeitenGuia Esvs Manejo Evc 2015Steeven Ruilova Valle100% (1)
- TugasDokument19 SeitenTugasaaNoch keine Bewertungen
- AMBOSS Study Guide for PLE Exam PreparationDokument77 SeitenAMBOSS Study Guide for PLE Exam PreparationFhai Escio100% (1)
- 2016 Pediatric RheumatologyDokument304 Seiten2016 Pediatric RheumatologyYudit Arenita100% (2)
- Pijl-2011-Longevity. The Allostatic Load of Dietary RestrictionDokument7 SeitenPijl-2011-Longevity. The Allostatic Load of Dietary RestrictionluizfernandosellaNoch keine Bewertungen
- The Pathophysiology of Otosclerosis: Review of Current ResearchDokument6 SeitenThe Pathophysiology of Otosclerosis: Review of Current ResearchFelipeAsenjoÁlvarezNoch keine Bewertungen
- World Health Organization: WHO/EMC/ZDI/98.6Dokument106 SeitenWorld Health Organization: WHO/EMC/ZDI/98.6ye yeNoch keine Bewertungen
- Acute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionVon EverandAcute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionNoch keine Bewertungen
- Wiersinga2016 ReferenceWorkEntry HashimotoSThyroiditisDokument44 SeitenWiersinga2016 ReferenceWorkEntry HashimotoSThyroiditisGaston ZamoranoNoch keine Bewertungen
- HPV-Infection and Cancers of the Skin - Diagnostics and TherapyVon EverandHPV-Infection and Cancers of the Skin - Diagnostics and TherapyBewertung: 5 von 5 Sternen5/5 (1)
- Who Might Be at RiskDokument5 SeitenWho Might Be at RiskichbinroelNoch keine Bewertungen
- Physio Test Do Not AnswerDokument75 SeitenPhysio Test Do Not AnswerAchraf RabadiNoch keine Bewertungen
- Guillain-Barré Syndrome: Understanding Epidemiology, Pathophysiology and ManagementDokument15 SeitenGuillain-Barré Syndrome: Understanding Epidemiology, Pathophysiology and ManagementindadzilarsyNoch keine Bewertungen
- AMBOSS 2021 ENAM Study GuideDokument49 SeitenAMBOSS 2021 ENAM Study GuideMadeline DelgadoNoch keine Bewertungen
- Serology PDFDokument201 SeitenSerology PDFGEBEYAW ADDISU100% (1)
- Bioequivalence Studies in Drug Development: Methods and ApplicationsVon EverandBioequivalence Studies in Drug Development: Methods and ApplicationsNoch keine Bewertungen
- Undergraduate Medicine Study Notes PDFDokument764 SeitenUndergraduate Medicine Study Notes PDFSHAKEEL1991Noch keine Bewertungen
- Chemotherapy and febrile neutropenia – Diagnostic and therapeutic managementVon EverandChemotherapy and febrile neutropenia – Diagnostic and therapeutic managementNoch keine Bewertungen
- Evidence-based Therapy of Psoriasis: Focus on BiologicsVon EverandEvidence-based Therapy of Psoriasis: Focus on BiologicsNoch keine Bewertungen
- Effects of Obesity On Depression A Role For Inflammation and The Gut MicrobiotaDokument8 SeitenEffects of Obesity On Depression A Role For Inflammation and The Gut MicrobiotaJerônimo CoelhoNoch keine Bewertungen
- Ca Colon 6Dokument28 SeitenCa Colon 6Tob JurNoch keine Bewertungen
- Guillain-Barr?? Syndrome: Epidemiology, Pathophysiology and ManagementDokument15 SeitenGuillain-Barr?? Syndrome: Epidemiology, Pathophysiology and Managementshf.mxlikNoch keine Bewertungen
- Journal of Affective Disorders: Giulio Perugi, Elie Hantouche, Giulia Vannucchi, Olavo PintoDokument15 SeitenJournal of Affective Disorders: Giulio Perugi, Elie Hantouche, Giulia Vannucchi, Olavo PintoLuigi Maria PandolfiNoch keine Bewertungen
- Bone Reports: Lisa Keung, Farzana Perwad TDokument8 SeitenBone Reports: Lisa Keung, Farzana Perwad Tfpm5948Noch keine Bewertungen
- Ni Hms 231894Dokument12 SeitenNi Hms 231894fpm5948Noch keine Bewertungen
- Thyroid Function in The Etiology of Fatigue in Breast CancerDokument15 SeitenThyroid Function in The Etiology of Fatigue in Breast Cancerfpm5948Noch keine Bewertungen
- Rubella Virus Replication and Links To TeratogenicityDokument17 SeitenRubella Virus Replication and Links To Teratogenicityfpm5948Noch keine Bewertungen
- Effect of Antioxidant Vitamins As Adjuvant Therapy For Sudden Sensorineural Hearing Loss: Systematic Review StudyDokument7 SeitenEffect of Antioxidant Vitamins As Adjuvant Therapy For Sudden Sensorineural Hearing Loss: Systematic Review Studyfpm5948Noch keine Bewertungen
- Further Efforts in The Achievement of Congenital Rubella Syndrome/rubella EliminationDokument5 SeitenFurther Efforts in The Achievement of Congenital Rubella Syndrome/rubella Eliminationfpm5948Noch keine Bewertungen
- 16Dokument3 Seiten16fpm5948Noch keine Bewertungen
- Ni Hms 835764Dokument16 SeitenNi Hms 835764fpm5948Noch keine Bewertungen
- Ni Hms 835764Dokument16 SeitenNi Hms 835764fpm5948Noch keine Bewertungen
- Fphys 06 00397Dokument11 SeitenFphys 06 00397fpm5948Noch keine Bewertungen
- Clinical Presentations of Parvovirus B19 InfectionDokument4 SeitenClinical Presentations of Parvovirus B19 Infectionfpm5948Noch keine Bewertungen
- Hand, Foot, and Mouth Disease Caused by Coxsackievirus A6: To The Editor: CoxsackievirusDokument3 SeitenHand, Foot, and Mouth Disease Caused by Coxsackievirus A6: To The Editor: Coxsackievirusfpm5948Noch keine Bewertungen
- Congenital Rubella Syndrome: The End Is in Sight: EditorialsDokument2 SeitenCongenital Rubella Syndrome: The End Is in Sight: Editorialsfpm5948Noch keine Bewertungen
- Pi Is 2352396415302334Dokument7 SeitenPi Is 2352396415302334fpm5948Noch keine Bewertungen
- NIH Public Access: Measles, Mumps, and RubellaDokument10 SeitenNIH Public Access: Measles, Mumps, and RubellaharryNoch keine Bewertungen
- V 37 N 3 A 08Dokument8 SeitenV 37 N 3 A 08fpm5948Noch keine Bewertungen
- B Jo 08700501Dokument20 SeitenB Jo 08700501fpm5948Noch keine Bewertungen
- Progress Toward Global Rubella Control and CRS PreventionDokument4 SeitenProgress Toward Global Rubella Control and CRS Preventionfpm5948Noch keine Bewertungen
- Coxsackievirus A16: Epidemiology, Diagnosis, and VaccineDokument8 SeitenCoxsackievirus A16: Epidemiology, Diagnosis, and Vaccinefpm5948Noch keine Bewertungen
- Cde 0005 0203Dokument7 SeitenCde 0005 0203fpm5948Noch keine Bewertungen
- Califmed00218 0008 PDFDokument4 SeitenCalifmed00218 0008 PDFfpm5948Noch keine Bewertungen
- S47 FullDokument10 SeitenS47 Fullfpm5948Noch keine Bewertungen
- Ecam2016 6075679Dokument6 SeitenEcam2016 6075679fpm5948Noch keine Bewertungen
- The Coxsackie Viruses : GilbertDokument4 SeitenThe Coxsackie Viruses : Gilbertfpm5948Noch keine Bewertungen
- S47 FullDokument10 SeitenS47 Fullfpm5948Noch keine Bewertungen
- Ijbms 17 929Dokument10 SeitenIjbms 17 929fpm5948Noch keine Bewertungen
- The Coxsackie Viruses : GilbertDokument4 SeitenThe Coxsackie Viruses : Gilbertfpm5948Noch keine Bewertungen
- 485Dokument21 Seiten485hectorNoch keine Bewertungen
- Nihms 73138 PDFDokument23 SeitenNihms 73138 PDFfpm5948Noch keine Bewertungen
- Neuropharmacological Effects of Nigella Sativa: Review ArticleDokument18 SeitenNeuropharmacological Effects of Nigella Sativa: Review Articlefpm5948Noch keine Bewertungen
- 19 Congenital HipotiroidDokument21 Seiten19 Congenital HipotiroidPande Indra PremanaNoch keine Bewertungen
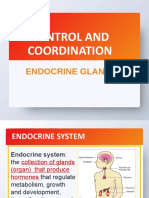
- Endocrine Glands and Their FunctionsDokument31 SeitenEndocrine Glands and Their FunctionsAfrina Asmi MINoch keine Bewertungen
- Youre Not Fat Youre Inflamed FINALDokument24 SeitenYoure Not Fat Youre Inflamed FINALSara Crespo100% (2)
- Marketing Channel Strategy 8th Edition Palmatier Solutions ManualDokument26 SeitenMarketing Channel Strategy 8th Edition Palmatier Solutions ManualStacyCarrgpjkb100% (49)
- Proefschrift Michel Weijerman 201011Dokument120 SeitenProefschrift Michel Weijerman 201011Nor HidayahNoch keine Bewertungen
- Endocrine Drugs: Pituitary, Thyroid, Parathyroid, and Adrenal DisordersDokument29 SeitenEndocrine Drugs: Pituitary, Thyroid, Parathyroid, and Adrenal DisordersPam LalaNoch keine Bewertungen
- Task 5 LQ (Mrs. Lizaveta)Dokument6 SeitenTask 5 LQ (Mrs. Lizaveta)çiğdem ünsalNoch keine Bewertungen
- Shashikant PDFDokument4 SeitenShashikant PDFAacharya Shashikant VashishthNoch keine Bewertungen
- Adrenal Fatigue: & Cortisol 101Dokument21 SeitenAdrenal Fatigue: & Cortisol 101Victoria D'Amico80% (5)
- MCQ Fracp 2002Dokument23 SeitenMCQ Fracp 2002mkuppam100% (1)
- Chapter 3 Essential Trace and Nonessential IonDokument8 SeitenChapter 3 Essential Trace and Nonessential IonAnthony V. DaquilaNoch keine Bewertungen
- Steps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-StepDokument9 SeitenSteps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Ahmad KamsyaDokument9 SeitenAhmad Kamsyaraynhard b. fandresNoch keine Bewertungen
- First Aid Q&A EmbryologyDokument13 SeitenFirst Aid Q&A EmbryologyzyadNoch keine Bewertungen
- Test - Surgery Book MCQs - Final Exam - QuizletDokument158 SeitenTest - Surgery Book MCQs - Final Exam - Quizlety SNoch keine Bewertungen
- Mrs Parveen Inamdar 29 02 2020 06 16 15 AM PDFDokument3 SeitenMrs Parveen Inamdar 29 02 2020 06 16 15 AM PDFmalhari katakdoundNoch keine Bewertungen
- Mineral DeficienciesDokument16 SeitenMineral DeficienciesDragan Pitic100% (4)
- Assessment of Serum Minerals and Electrolytes in TDokument5 SeitenAssessment of Serum Minerals and Electrolytes in THasni M MarsaolyNoch keine Bewertungen
- Endocrine Gland Disorders and MetabolismDokument74 SeitenEndocrine Gland Disorders and MetabolismRatnam hospitalNoch keine Bewertungen
- Endocrine ResonanceDokument51 SeitenEndocrine ResonanceEkta ManglaniNoch keine Bewertungen
- Lecture 2 GoiterDokument3 SeitenLecture 2 GoiterKarizma TravelNoch keine Bewertungen
- Thyroid Storm: Karthik Balachandran Karthik2k2Dokument52 SeitenThyroid Storm: Karthik Balachandran Karthik2k2Dr Karthik Balachandran, EndocrinologyNoch keine Bewertungen
- Blood and TSH ReportDokument3 SeitenBlood and TSH Reportindrajit sinhaNoch keine Bewertungen
- Thyroid CancerDokument38 SeitenThyroid CancerNinikNoch keine Bewertungen
- Review of Ayurvedic Drugs Acting On Hypothyroidism: Tarun Sharma, Malvika, Monu Gupta, Sumit NathaniDokument8 SeitenReview of Ayurvedic Drugs Acting On Hypothyroidism: Tarun Sharma, Malvika, Monu Gupta, Sumit NathaniVakamalla SubbareddyNoch keine Bewertungen
- Grace - HyperthyroidismDokument9 SeitenGrace - HyperthyroidismOkoro Tochukwu ProsperNoch keine Bewertungen
- Endocrinology PathophysiologyDokument136 SeitenEndocrinology PathophysiologyDaniel DiasNoch keine Bewertungen
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDokument2 SeitenDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNoch keine Bewertungen
- Parathyroid Scintigraphy: A Technologist's GuideDokument44 SeitenParathyroid Scintigraphy: A Technologist's GuidePatricia MeloNoch keine Bewertungen
- Thyroid Stimulating Hormone Test and Its Effect On The Human BodyDokument4 SeitenThyroid Stimulating Hormone Test and Its Effect On The Human BodyInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen