Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Anatomy Final Exam Notes PDFDokument45 SeitenAnatomy Final Exam Notes PDFLydia LalalandNoch keine Bewertungen
- English FAQ v3 PDFDokument26 SeitenEnglish FAQ v3 PDFibrahim 12Noch keine Bewertungen
- Speaking Checklist Glossary Updated Speaking 2018Dokument5 SeitenSpeaking Checklist Glossary Updated Speaking 2018Gamaliel VentoNoch keine Bewertungen
- How To Make Dakin's Solution: SuppliesDokument2 SeitenHow To Make Dakin's Solution: Suppliesbradley_brown_1Noch keine Bewertungen
- Glasgow Coma Scale Assessment Tool ExplainedDokument41 SeitenGlasgow Coma Scale Assessment Tool ExplainedCharmaine Kayzhel UmaliNoch keine Bewertungen
- DKA ProtocolDokument3 SeitenDKA Protocolpinky222255554100% (1)
- Eeg Reading TipsDokument6 SeitenEeg Reading TipsJULIENoch keine Bewertungen
- Experienced Filipino OR Nurse Seeks New OpportunitiesDokument4 SeitenExperienced Filipino OR Nurse Seeks New OpportunitiesJohn Dela CruzNoch keine Bewertungen
- Charmaine Kayzhel Umali ResumeDokument2 SeitenCharmaine Kayzhel Umali ResumeCharmaine Kayzhel UmaliNoch keine Bewertungen
- Fluid intake and output chart summaryDokument1 SeiteFluid intake and output chart summaryCharmaine Kayzhel UmaliNoch keine Bewertungen
- John Green QuotesDokument23 SeitenJohn Green QuotesCharmaine Kayzhel UmaliNoch keine Bewertungen
- 63 Must Know Lab Values Cheat Sheet - NCLEX (Caribbean Nurses of Puerto Rico and Latin America) PDFDokument4 Seiten63 Must Know Lab Values Cheat Sheet - NCLEX (Caribbean Nurses of Puerto Rico and Latin America) PDFChristineBiankii100% (1)
- TuberculosisDokument31 SeitenTuberculosisCharmaine Kayzhel UmaliNoch keine Bewertungen
- Holistic Assessment For Hiring Effective Nursing StaffDokument18 SeitenHolistic Assessment For Hiring Effective Nursing StaffCharmaine Kayzhel UmaliNoch keine Bewertungen
- Holistic Assessment For Hiring Effective Nursing StaffDokument18 SeitenHolistic Assessment For Hiring Effective Nursing StaffCharmaine Kayzhel UmaliNoch keine Bewertungen
- Case Study RespiDokument4 SeitenCase Study RespiCharmaine Kayzhel UmaliNoch keine Bewertungen
- Eeg Reading TipsDokument6 SeitenEeg Reading TipsJULIENoch keine Bewertungen
- Pages From LolitaDokument10 SeitenPages From LolitaCharmaine Kayzhel UmaliNoch keine Bewertungen
- Contemplation of BeautyDokument19 SeitenContemplation of BeautyCharmaine Kayzhel UmaliNoch keine Bewertungen
- Phil PassportDokument2 SeitenPhil PassportCharmaine Kayzhel UmaliNoch keine Bewertungen
- Developmental Milestones: Prepared By: John Gil B. Ricafort, RNDokument21 SeitenDevelopmental Milestones: Prepared By: John Gil B. Ricafort, RNCharmaine Kayzhel UmaliNoch keine Bewertungen
- Quotes From Mara DyerDokument10 SeitenQuotes From Mara DyerCharmaine Kayzhel UmaliNoch keine Bewertungen
- Nle Application Sample FormDokument2 SeitenNle Application Sample FormCharmaine Kayzhel UmaliNoch keine Bewertungen
- Contemplation of BeautyDokument19 SeitenContemplation of BeautyCharmaine Kayzhel UmaliNoch keine Bewertungen
- Nle Application Sample FormDokument2 SeitenNle Application Sample FormCharmaine Kayzhel UmaliNoch keine Bewertungen
- The Concept of Platonic LoveDokument59 SeitenThe Concept of Platonic LoveSham ShamkarNoch keine Bewertungen
- Trivia FactsDokument51 SeitenTrivia Factsapi-3713843100% (5)
- VitaminDokument2 SeitenVitaminCharmaine Kayzhel UmaliNoch keine Bewertungen
- The Contemplation of Beauty Causes The Soul To Sprout WingsDokument21 SeitenThe Contemplation of Beauty Causes The Soul To Sprout WingsCharmaine Kayzhel UmaliNoch keine Bewertungen
- Se Ques Trec To My (S KW - STR K T - M) Surgical Removal of A SequestrumDokument1 SeiteSe Ques Trec To My (S KW - STR K T - M) Surgical Removal of A SequestrumCharmaine Kayzhel UmaliNoch keine Bewertungen
- Why study Physical Education in collegeDokument48 SeitenWhy study Physical Education in collegeM-jay BarnobalNoch keine Bewertungen
- A House Officer's Approach To DengueDokument9 SeitenA House Officer's Approach To DengueBaihaqi SaharunNoch keine Bewertungen
- Jha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseDokument5 SeitenJha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseProdi Bedah SarafNoch keine Bewertungen
- WSES Consensus Conference Guidelines - TCEDokument9 SeitenWSES Consensus Conference Guidelines - TCEDr. Victor Alonso Hernández HernándezNoch keine Bewertungen
- Blood Pressure and Pulse RateDokument7 SeitenBlood Pressure and Pulse Ratehjaffer2001100% (1)
- Kasturi Sonawane - FYReportDokument62 SeitenKasturi Sonawane - FYReportKasturi SonawaneNoch keine Bewertungen
- Stuffed NurseDokument42 SeitenStuffed NurseG-s HO CKNoch keine Bewertungen
- Complete HH May 2020Dokument60 SeitenComplete HH May 2020BruntNoch keine Bewertungen
- Medical Emergencies in Rehabilitation MedicineDokument24 SeitenMedical Emergencies in Rehabilitation MedicineAzza El Awar100% (1)
- Ge - Carescape Monitor b650 v2 - User ManualDokument536 SeitenGe - Carescape Monitor b650 v2 - User ManualrichsalgadoNoch keine Bewertungen
- Heart disease in pregnancyDokument87 SeitenHeart disease in pregnancyMonisha ArulalanNoch keine Bewertungen
- Constrictive PericarditisDokument54 SeitenConstrictive PericarditisRazib AlamNoch keine Bewertungen
- A. Fisiologi RespirasiDokument77 SeitenA. Fisiologi RespirasiasriNoch keine Bewertungen
- Aromaterapi Rose Terhadap Penurunan TD Pada MenopauseDokument6 SeitenAromaterapi Rose Terhadap Penurunan TD Pada MenopauseDesi Fitri AyuniNoch keine Bewertungen
- Principles and Techniques of Blood Pressure MeasurementDokument26 SeitenPrinciples and Techniques of Blood Pressure MeasurementWagnerNoch keine Bewertungen
- FLUKE ProSim 8 Technical DataDokument12 SeitenFLUKE ProSim 8 Technical DataZurab SanikidzeNoch keine Bewertungen
- Dr. Warsinggih, SP.B-KBD (SLIDE ERAS in Digestive Surgery)Dokument34 SeitenDr. Warsinggih, SP.B-KBD (SLIDE ERAS in Digestive Surgery)dewiswahyuNoch keine Bewertungen
- Accommodation Management 5th Sem. Notes by Kirti PuriDokument25 SeitenAccommodation Management 5th Sem. Notes by Kirti PuriAmit MondalNoch keine Bewertungen
- C - Cardiovascular PhysiologyDokument61 SeitenC - Cardiovascular PhysiologyMohamad Zekry ZuhairyNoch keine Bewertungen
- Cardiovascular ExaminationDokument127 SeitenCardiovascular Examinationwakemeup143Noch keine Bewertungen
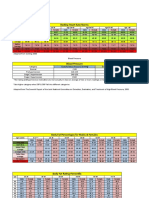
- Resting Heart Rate NormsDokument3 SeitenResting Heart Rate Normstre100% (1)
- Jurnal Biokimia KalsiumDokument5 SeitenJurnal Biokimia KalsiumdimitriprawiraNoch keine Bewertungen
- BP 2018Dokument7 SeitenBP 2018Rafael MeloNoch keine Bewertungen
- Test Bank For Basic Medical Language 4th Edition Lafleur DownloadDokument13 SeitenTest Bank For Basic Medical Language 4th Edition Lafleur Downloadantoniowagnercrqampebwt100% (28)
- The Effect of Ergonomic Exercise On Changes in Blood Pressure in Patients With HypertensionDokument11 SeitenThe Effect of Ergonomic Exercise On Changes in Blood Pressure in Patients With HypertensionRizky MocinNoch keine Bewertungen
- CDH and Pulmonary HypertensionDokument6 SeitenCDH and Pulmonary HypertensionStollery SandboxNoch keine Bewertungen
- Vital SignsDokument97 SeitenVital SignsPrincess Mariscotes100% (1)
- UntitledDokument20 SeitenUntitledJhon Kenneth Magalong JuguilonNoch keine Bewertungen
- Critical Care of The Burned PatientDokument222 SeitenCritical Care of The Burned PatientYunita Manurung100% (1)