Das könnte Ihnen auch gefallen
- INventory Management at Health CareDokument33 SeitenINventory Management at Health CareishabihNoch keine Bewertungen
- SCM in HealthcareDokument9 SeitenSCM in HealthcareAnurag GuptaNoch keine Bewertungen
- Supply Chain Management in Healthcare IndustryDokument4 SeitenSupply Chain Management in Healthcare IndustryInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDokument23 SeitenWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDiahNoch keine Bewertungen
- Silo - Tips - Supply Chain Management in Hospital A Case StudyDokument7 SeitenSilo - Tips - Supply Chain Management in Hospital A Case Study398Rishabh RajNoch keine Bewertungen
- Supply Chain Management Practice in Clinical Pharmacy: A Case StudyDokument9 SeitenSupply Chain Management Practice in Clinical Pharmacy: A Case Studyrragbir35Noch keine Bewertungen
- New Trends in Supply ChainDokument12 SeitenNew Trends in Supply Chaindeepti ramdinNoch keine Bewertungen
- Healthcare Supply Chain Management in Malaysia: A Case StudyDokument11 SeitenHealthcare Supply Chain Management in Malaysia: A Case StudyPulkit BhardwajNoch keine Bewertungen
- Inventory Management of Medical Consumables in Public Hospital: A Case StudyDokument6 SeitenInventory Management of Medical Consumables in Public Hospital: A Case Studybagyi111Noch keine Bewertungen
- Hospital LogsDokument6 SeitenHospital LogsDavid SetiawanNoch keine Bewertungen
- Health Care MGTDokument13 SeitenHealth Care MGTRicha SinghNoch keine Bewertungen
- Inventory Management Issues in Health Care SupplyDokument34 SeitenInventory Management Issues in Health Care SupplyYogesh ChandraNoch keine Bewertungen
- Reducing Waste in ICUDokument10 SeitenReducing Waste in ICUzorbini69Noch keine Bewertungen
- Healthcare Supply ChainDokument351 SeitenHealthcare Supply ChainLiêm LaNoch keine Bewertungen
- Hall Flows Hospitals Chapter1text PDFDokument45 SeitenHall Flows Hospitals Chapter1text PDFShin BoyceNoch keine Bewertungen
- Collaborative Implementation of E-Business Processes Within The Health-Care Supply ChainDokument10 SeitenCollaborative Implementation of E-Business Processes Within The Health-Care Supply ChainEmmy SukhNoch keine Bewertungen
- Chapter 11. Supply Chain & Inventory ManagementDokument47 SeitenChapter 11. Supply Chain & Inventory ManagementAli ElattarNoch keine Bewertungen
- Innovative ExperienceDokument17 SeitenInnovative ExperienceliliNoch keine Bewertungen
- Supply Chain Management in The Healthcare IndustryDokument23 SeitenSupply Chain Management in The Healthcare IndustryMohammed Al Ayoubi67% (3)
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationVon EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationNoch keine Bewertungen
- Dr. Martin's OfficeDokument4 SeitenDr. Martin's OfficeCheryl CastanedaNoch keine Bewertungen
- Supply Chain Inventory ManagementDokument46 SeitenSupply Chain Inventory ManagementMUKESH SUNDARARAJANNoch keine Bewertungen
- Supply Documentation at The POUDokument13 SeitenSupply Documentation at The POURaghavendra KuthadiNoch keine Bewertungen
- Inventory ManagementDokument9 SeitenInventory ManagementShikhaNoch keine Bewertungen
- Mining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingVon EverandMining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingNoch keine Bewertungen
- Streamlining Distribution in The Pharmaceutical Industry: Life SciencesDokument16 SeitenStreamlining Distribution in The Pharmaceutical Industry: Life SciencesBalaji RamasubramanianNoch keine Bewertungen
- Healthcare SCM in Malaysia - Case StudyDokument10 SeitenHealthcare SCM in Malaysia - Case StudyHussain Alam100% (1)
- Logistics in Hospitals: A Case Study of Some Singapore HospitalsDokument13 SeitenLogistics in Hospitals: A Case Study of Some Singapore HospitalsSapta YudhaNoch keine Bewertungen
- Summary2017 08-MedicalEquipmentDokument6 SeitenSummary2017 08-MedicalEquipmentAshish ChauhanNoch keine Bewertungen
- Not Your Fathers Supply ChainDokument4 SeitenNot Your Fathers Supply Chainkhadden999Noch keine Bewertungen
- Quality Assurance in Humanitarian Medical Supply ChainsDokument33 SeitenQuality Assurance in Humanitarian Medical Supply ChainsDennis BoursNoch keine Bewertungen
- Gha 8 26546Dokument10 SeitenGha 8 26546proneigrihmsNoch keine Bewertungen
- 7 Ps HospitalsDokument6 Seiten7 Ps Hospitalsamb aniNoch keine Bewertungen
- Supply Chain-HospitalDokument6 SeitenSupply Chain-Hospitalmusa alisabanaNoch keine Bewertungen
- Important of Supply Chain Management in Healthcare OrganizationDokument3 SeitenImportant of Supply Chain Management in Healthcare OrganizationAhmed KabirNoch keine Bewertungen
- Pengantar Manajemen Logistik Farmasi RS PDFDokument25 SeitenPengantar Manajemen Logistik Farmasi RS PDFgithaNoch keine Bewertungen
- Integrity of The Pharmaceutical Supply Chain:: Product Sourcing For Patient SafetyDokument10 SeitenIntegrity of The Pharmaceutical Supply Chain:: Product Sourcing For Patient SafetymurugananthCNoch keine Bewertungen
- Apa AjasdsdsdsadsdsadsdadasdasdasddasdsdsadDokument15 SeitenApa AjasdsdsdsadsdsadsdadasdasdasddasdsdsadIrwan WijayaNoch keine Bewertungen
- Aptel PDFDokument26 SeitenAptel PDFlovita dibaNoch keine Bewertungen
- Pharmaceutical Supply Chain and Inventory Management Strategies PDFDokument13 SeitenPharmaceutical Supply Chain and Inventory Management Strategies PDFRizky AzizahNoch keine Bewertungen
- Read HHS Inspector General's ReportDokument41 SeitenRead HHS Inspector General's Reportkballuck1Noch keine Bewertungen
- HHS Inspector General Report Covid 19 Oei-06!20!00300Dokument41 SeitenHHS Inspector General Report Covid 19 Oei-06!20!00300Douglas PierreNoch keine Bewertungen
- Hospital Experiences Responding To The COVID-19 PandemicDokument41 SeitenHospital Experiences Responding To The COVID-19 PandemicLaw&CrimeNoch keine Bewertungen
- Managing Medicines in The Hospital Pharmacy: Logistics InefficienciesDokument6 SeitenManaging Medicines in The Hospital Pharmacy: Logistics InefficienciesElsaNoch keine Bewertungen
- Hospital & Healthcare IndustryDokument25 SeitenHospital & Healthcare IndustryManish PooniaNoch keine Bewertungen
- Guidelines For ICU Admission, Discharge, and Triage (Crit Care Med 1999)Dokument11 SeitenGuidelines For ICU Admission, Discharge, and Triage (Crit Care Med 1999)Kary VelazquezNoch keine Bewertungen
- CP Driving High Reliability and High ValueDokument12 SeitenCP Driving High Reliability and High ValueAkhmad IrawanNoch keine Bewertungen
- Michael Porter's Value-Based Health Care Delivery ProposalDokument14 SeitenMichael Porter's Value-Based Health Care Delivery Proposalvadmanh100% (1)
- Business Analytics: Hospital - Facilities Management and Utilisation For A 100 Bedded HospitalDokument44 SeitenBusiness Analytics: Hospital - Facilities Management and Utilisation For A 100 Bedded HospitalAswani AbayanNoch keine Bewertungen
- Shifting The Balance of Care Report Web FinalDokument139 SeitenShifting The Balance of Care Report Web Finalvivek.nanda7292Noch keine Bewertungen
- Coordinating Health ServicesDokument25 SeitenCoordinating Health ServicesbdivanNoch keine Bewertungen
- Rating Methodology-Hospitals - August2020Dokument6 SeitenRating Methodology-Hospitals - August2020Neelaj MaityNoch keine Bewertungen
- United States Resource Availability For COVID-19: Statistics On Critical Care With This New Document Focusing ResourcesDokument16 SeitenUnited States Resource Availability For COVID-19: Statistics On Critical Care With This New Document Focusing ResourcesPurwadi SujalmoNoch keine Bewertungen
- Rating Methodology - Hospitals - 11aug2020Dokument6 SeitenRating Methodology - Hospitals - 11aug2020Akshit AggarwalNoch keine Bewertungen
- CH-1 Hospital and Their OrganizationDokument11 SeitenCH-1 Hospital and Their OrganizationrevaNoch keine Bewertungen
- AmbulatoryDokument6 SeitenAmbulatorysusan_grace123Noch keine Bewertungen
- f3d3 PDFDokument40 Seitenf3d3 PDFSiti QamariaNoch keine Bewertungen
- Health Care Value ChainDokument24 SeitenHealth Care Value ChainallisterotherNoch keine Bewertungen
- Cognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareVon EverandCognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareKai ZhengNoch keine Bewertungen
- Therapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyVon EverandTherapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyNoch keine Bewertungen
- Mad 1-2-3 PMDokument33 SeitenMad 1-2-3 PMK.B.SNoch keine Bewertungen
- Ebook - Allan Mckay - VFX Hardware Guide - Jan 2019 PDFDokument29 SeitenEbook - Allan Mckay - VFX Hardware Guide - Jan 2019 PDFSundeep ParmarNoch keine Bewertungen
- Java Exam Preparation Practice Test - 1Dokument10 SeitenJava Exam Preparation Practice Test - 1mziabdNoch keine Bewertungen
- Lecture0 720p enDokument19 SeitenLecture0 720p enanupathi mamatha deen dayalNoch keine Bewertungen
- Advanced Strategic ManagementDokument110 SeitenAdvanced Strategic ManagementDr Rushen SinghNoch keine Bewertungen
- Surat Pernyataan Calon Mahasiswa BaruDokument3 SeitenSurat Pernyataan Calon Mahasiswa Barua2020-11469 Ian Hadisurya BudimanNoch keine Bewertungen
- Arts 6 - Q4 - M1Dokument15 SeitenArts 6 - Q4 - M1Joed WayasNoch keine Bewertungen
- Li4278 Spec Sheet en UsDokument2 SeitenLi4278 Spec Sheet en UsErwin RamadhanNoch keine Bewertungen
- CCNP Switching LAB Preparation TestDokument2 SeitenCCNP Switching LAB Preparation TestGiannisDemetriouNoch keine Bewertungen
- Style Master For Keyboard PerformersDokument25 SeitenStyle Master For Keyboard PerformerskbdinfinityNoch keine Bewertungen
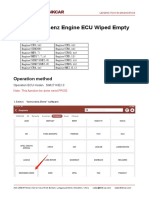
- Mercedes Benz Engine ECU Wiped EmptyDokument9 SeitenMercedes Benz Engine ECU Wiped EmptyP BNoch keine Bewertungen
- Tomorrow'S Technology For Today'S Security: Product HighlightsDokument2 SeitenTomorrow'S Technology For Today'S Security: Product HighlightsBanu AtamNoch keine Bewertungen
- Cartilla Informativa Plan LectorDokument11 SeitenCartilla Informativa Plan LectorHilarioPaniuraHuayhuaNoch keine Bewertungen
- Job Description PharmacistDokument4 SeitenJob Description PharmacistAbdiNoch keine Bewertungen
- QXDM Filters For UE IssuesDokument4 SeitenQXDM Filters For UE Issuessandeepdhariwal7661Noch keine Bewertungen
- The Importance of Basic Printing Education For Human Resource Development in Printing IndustryDokument12 SeitenThe Importance of Basic Printing Education For Human Resource Development in Printing IndustryAries Chandra AnandithaNoch keine Bewertungen
- Technovision Technovision: Simplify SimplifyDokument86 SeitenTechnovision Technovision: Simplify SimplifySayandip SarkarNoch keine Bewertungen
- CNATRAINST 1542.195 Chief Naval Air Training Primary Pilot TrainingDokument164 SeitenCNATRAINST 1542.195 Chief Naval Air Training Primary Pilot Trainingmuttley jones2Noch keine Bewertungen
- Assignment On VOIPDokument5 SeitenAssignment On VOIPRayan KarimNoch keine Bewertungen
- Sentiment Analysis of Stock News Using NLTKDokument6 SeitenSentiment Analysis of Stock News Using NLTKVIVA-TECH IJRINoch keine Bewertungen
- What Are The Three Ways That Computer Buses Can Be Used To Communicate With Memory and I/O?Dokument1 SeiteWhat Are The Three Ways That Computer Buses Can Be Used To Communicate With Memory and I/O?Safa MNoch keine Bewertungen
- Converting To SAP S/4HANA: Custom Code MigrationDokument15 SeitenConverting To SAP S/4HANA: Custom Code MigrationKevin AndersonNoch keine Bewertungen
- Test Point Insertion For Test Coverage Improvement in DFT - Design For Testability (DFT) .HTMLDokument75 SeitenTest Point Insertion For Test Coverage Improvement in DFT - Design For Testability (DFT) .HTMLIlaiyaveni IyanduraiNoch keine Bewertungen
- MAC-LAB Transfer Operator's ManualDokument37 SeitenMAC-LAB Transfer Operator's ManualAbdelhakszn SznNoch keine Bewertungen
- ELL782: Computer ArchitectureDokument2 SeitenELL782: Computer ArchitectureSIYAB KhanNoch keine Bewertungen
- Artificial Int Text BookDokument100 SeitenArtificial Int Text BookAshwinNoch keine Bewertungen
- Chapter1-Nature of StatisticsDokument10 SeitenChapter1-Nature of StatisticsNelia Olaso InsonNoch keine Bewertungen
- Material de Referencia - IT4IT™ Foundation Study GuideDokument176 SeitenMaterial de Referencia - IT4IT™ Foundation Study Guidedagomez2013Noch keine Bewertungen
- Current Transformers How To Specify Them PDFDokument36 SeitenCurrent Transformers How To Specify Them PDFargari19Noch keine Bewertungen
- DVB-RCS NCR SPTDokument8 SeitenDVB-RCS NCR SPTMike millyNoch keine Bewertungen