Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Askep Kritis Sistem EndokrinDokument37 SeitenAskep Kritis Sistem EndokrinDerfina Bahagia iduNoch keine Bewertungen
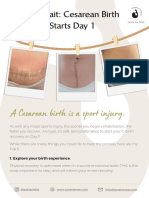
- C-Section RecoveryDokument3 SeitenC-Section RecoveryClaudia IndrieNoch keine Bewertungen
- Yale Insulin Infusion ProtocolDokument2 SeitenYale Insulin Infusion ProtocolIffatNaeemNoch keine Bewertungen
- Hospital Teams: Bahasa InggrisDokument6 SeitenHospital Teams: Bahasa InggrisIlhamNoch keine Bewertungen
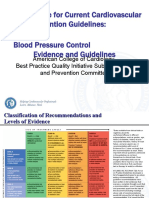
- 3 ACC Prevention Blood PressureDokument69 Seiten3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- Accesiblities of Accadamic For Students With Dis AblitiesDokument8 SeitenAccesiblities of Accadamic For Students With Dis AblitiesGuutaa DirbabaaNoch keine Bewertungen
- Type 1 Diabetes Mellitus Workup - Laboratory Studies, Tests To Differentiate Type 1 From Type 2 DiabetesDokument3 SeitenType 1 Diabetes Mellitus Workup - Laboratory Studies, Tests To Differentiate Type 1 From Type 2 DiabetesTrifosa Ika Septiana EryaniNoch keine Bewertungen
- High Voltage Galvanic Current Lecture PDFDokument22 SeitenHigh Voltage Galvanic Current Lecture PDFdespNoch keine Bewertungen
- General Properties of CestodesDokument42 SeitenGeneral Properties of CestodesNicole NipasNoch keine Bewertungen
- Oral PathologyDokument31 SeitenOral PathologyAnonymous GyqTkXMwMNoch keine Bewertungen
- Amisulprid 2Dokument5 SeitenAmisulprid 2Robert MovileanuNoch keine Bewertungen
- Pasteur Vs Bechamp - An Alternative View of Infectious DiseaseDokument3 SeitenPasteur Vs Bechamp - An Alternative View of Infectious DiseaseRadhe GovindaNoch keine Bewertungen
- Teaching Practice.... Lung CancerDokument32 SeitenTeaching Practice.... Lung CancernamitaNoch keine Bewertungen
- 06 Clinical Pathology MCQs With Answers 1Dokument29 Seiten06 Clinical Pathology MCQs With Answers 1Habib Ullah100% (1)
- Treatment of Hyponatremia - Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and Reset OsmostatDokument15 SeitenTreatment of Hyponatremia - Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and Reset Osmostathoneyworks100% (1)
- 53 Coronary Artery AnomaliesDokument5 Seiten53 Coronary Artery AnomaliesVictor PazNoch keine Bewertungen
- Female Genital Tract Cytopathology: PracticalDokument26 SeitenFemale Genital Tract Cytopathology: PracticalNgotelo FunwiNoch keine Bewertungen
- Feline Anemia Diagnostic AlgorithmDokument1 SeiteFeline Anemia Diagnostic AlgorithmEd BlackadderNoch keine Bewertungen
- EAU Pocket On Paediatric Urology 2023Dokument54 SeitenEAU Pocket On Paediatric Urology 2023Andrea SzaszNoch keine Bewertungen
- Rectal ProlapseDokument2 SeitenRectal ProlapseSalem ZoghbyNoch keine Bewertungen
- EAU 2022 - Prostate CancerDokument229 SeitenEAU 2022 - Prostate Cancerpablo penguinNoch keine Bewertungen
- Public Health COC ExamDokument19 SeitenPublic Health COC ExamTut Kong RuachNoch keine Bewertungen
- Geriatric OtolaryngologyDokument26 SeitenGeriatric OtolaryngologySari RakhmawatiNoch keine Bewertungen
- L17. Askep Kritis Dan Gadar Pasien Dengan Ggguan Sistem Pernafan NontraumatikDokument75 SeitenL17. Askep Kritis Dan Gadar Pasien Dengan Ggguan Sistem Pernafan NontraumatikSepto KristianaNoch keine Bewertungen
- FNCP - Inadequate Exercise & Breeding Site For MosquitoesDokument2 SeitenFNCP - Inadequate Exercise & Breeding Site For MosquitoesGwyneth Fisher100% (1)
- Late Pregnancy Bleeding (LPB) : Antepartum Hemorrhage (Aph) Dr. A. MutungiDokument3 SeitenLate Pregnancy Bleeding (LPB) : Antepartum Hemorrhage (Aph) Dr. A. Mutungikhadzx100% (2)
- PRECIO PromalabDokument6 SeitenPRECIO PromalabJenny QuingaNoch keine Bewertungen
- Office: of The SecretaryDokument7 SeitenOffice: of The SecretaryFidelis MaximusNoch keine Bewertungen
- The Impact of Lifestyle Interventions On Type 2 Diabetes Management, A Comprehensive AnalysisDokument2 SeitenThe Impact of Lifestyle Interventions On Type 2 Diabetes Management, A Comprehensive AnalysisJohn nyoikeNoch keine Bewertungen
- Level 3 Body Sleep - Sample ReportDokument6 SeitenLevel 3 Body Sleep - Sample Reportjunior browNoch keine Bewertungen