Das könnte Ihnen auch gefallen
- Tips Sa Boards TextsDokument3 SeitenTips Sa Boards Textshallegail100% (1)
- Topnotch ECG Interpretation For MoonlightersDokument25 SeitenTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- Patho Supplement Handout For Sept 2018 UPDATED May 2018 PDFDokument25 SeitenPatho Supplement Handout For Sept 2018 UPDATED May 2018 PDFemely p. tango100% (1)
- PRC ObDokument20 SeitenPRC ObLian BaylosisNoch keine Bewertungen
- Topnotch Pediatrics For MoonlightersDokument323 SeitenTopnotch Pediatrics For Moonlightersmefav7778520100% (1)
- TOPNOTCH Microbiology-Supertable-by-Dr - Cocoy-Calderon-Jaffar-Pineda-Troy-Soberano-UPDATED-NOVEMBER-2017 PDFDokument34 SeitenTOPNOTCH Microbiology-Supertable-by-Dr - Cocoy-Calderon-Jaffar-Pineda-Troy-Soberano-UPDATED-NOVEMBER-2017 PDFWaiwit KritayakiranaNoch keine Bewertungen
- Review TipsDokument5 SeitenReview TipsyanafkNoch keine Bewertungen
- Topnotch Microbiology Supertable UPDATED Jan 2016 by DR - Cocoy Calderon PDFDokument75 SeitenTopnotch Microbiology Supertable UPDATED Jan 2016 by DR - Cocoy Calderon PDFDre Valdez100% (1)
- September 2021 PleDokument20 SeitenSeptember 2021 PleGian PagadduNoch keine Bewertungen
- SurgeryDokument40 SeitenSurgerychristine_8995Noch keine Bewertungen
- Preventive Medicine PLE ReviewerDokument4 SeitenPreventive Medicine PLE ReviewerReinhard Ivan MansibangNoch keine Bewertungen
- PLE Microbiology Cheat SheetDokument2 SeitenPLE Microbiology Cheat SheetModesto Gallardo100% (1)
- Hi-Yield Notes in Im & PediaDokument20 SeitenHi-Yield Notes in Im & PediaJohn Christopher LucesNoch keine Bewertungen
- BOARD EXAM BooksDokument2 SeitenBOARD EXAM BooksLuka Desabelle- JustoNoch keine Bewertungen
- Topnotch Mnemonics - September 2016Dokument6 SeitenTopnotch Mnemonics - September 2016JB ReyesNoch keine Bewertungen
- University of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - ConsortiumDokument17 SeitenUniversity of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - Consortiummefav7778520Noch keine Bewertungen
- Hi-Yield Notes in Legal MedDokument16 SeitenHi-Yield Notes in Legal MedJohn Christopher Luces100% (1)
- Physician Licensure Exam March 2019 Recall: MicrobiologyDokument4 SeitenPhysician Licensure Exam March 2019 Recall: MicrobiologyNica Lopez FernandezNoch keine Bewertungen
- PLE Recall March 2016Dokument13 SeitenPLE Recall March 2016Lian BaylosisNoch keine Bewertungen
- Topnotch Microbiology Supertable - by DR - Cocoy Calderon, Jaffar Pineda, Troy SoberanoDokument3 SeitenTopnotch Microbiology Supertable - by DR - Cocoy Calderon, Jaffar Pineda, Troy SoberanoJohn Christopher Luces100% (1)
- Pathology Ple SamplexDokument5 SeitenPathology Ple SamplexdawnparkNoch keine Bewertungen
- Topnotch Surgery Supplement HandoutDokument85 SeitenTopnotch Surgery Supplement HandoutSarah Michelle NiduaNoch keine Bewertungen
- Topnotch Ent Supplement Handout Updated April 2016pdf PDFDokument15 SeitenTopnotch Ent Supplement Handout Updated April 2016pdf PDFKenneth NuñezNoch keine Bewertungen
- 4 Physiology Supplement Handout Based On Ganong For TOPNOTCH 21 by Jaffar PinedaDokument46 Seiten4 Physiology Supplement Handout Based On Ganong For TOPNOTCH 21 by Jaffar PinedaAthena Borja100% (3)
- 9a Pathology PDFDokument47 Seiten9a Pathology PDFDianne GalangNoch keine Bewertungen
- Final Coaching - Im 2022Dokument9 SeitenFinal Coaching - Im 2022Jhon PauloNoch keine Bewertungen
- TOPNOTCH Pathology Pearls September 2018 PDFDokument18 SeitenTOPNOTCH Pathology Pearls September 2018 PDFNica Lopez FernandezNoch keine Bewertungen
- Final Coaching - Obgyne 2022Dokument7 SeitenFinal Coaching - Obgyne 2022Jhon PauloNoch keine Bewertungen
- Topnotch Surgery Reviewer PDFDokument81 SeitenTopnotch Surgery Reviewer PDFMarie Frances Lalican-Ringel100% (16)
- PRC QuestionsDokument45 SeitenPRC QuestionsJohn Christopher Luces100% (2)
- Topnotch IM For MoonlightersDokument274 SeitenTopnotch IM For Moonlightersmefav7778520100% (2)
- Feb 2015 Physician Licensure ExamDokument1 SeiteFeb 2015 Physician Licensure ExamyanafkNoch keine Bewertungen
- Pathology PRC FinaleditDokument11 SeitenPathology PRC FinaleditVince Cabahug100% (1)
- Er Meds: DiclofenacDokument3 SeitenEr Meds: Diclofenacmefav7778520Noch keine Bewertungen
- 9 Topnotch Internal Medicine Superexampdf PDFDokument95 Seiten9 Topnotch Internal Medicine Superexampdf PDFSheryl Layne Lao-Sebrio100% (1)
- Hi-Yield Notes in SurgeryDokument18 SeitenHi-Yield Notes in SurgeryJohn Christopher Luces50% (2)
- Internal Medicine Ple ReviewerDokument7 SeitenInternal Medicine Ple ReviewerReinhard Ivan MansibangNoch keine Bewertungen
- #ROADTOPLE An Almost Complete Guide To The... - Chloramphenicole - MD - Facebook PDFDokument10 Seiten#ROADTOPLE An Almost Complete Guide To The... - Chloramphenicole - MD - Facebook PDFJoy FucananNoch keine Bewertungen
- A Brief Guide To The Physician Licensure ExaminationDokument31 SeitenA Brief Guide To The Physician Licensure ExaminationAb Hermoso100% (1)
- Topnotch Pathology Supplemental PICTURES Powerpoint Based On Handouts September 2019Dokument53 SeitenTopnotch Pathology Supplemental PICTURES Powerpoint Based On Handouts September 2019croixNoch keine Bewertungen
- Topnotch Surgery Reviewer PDFDokument81 SeitenTopnotch Surgery Reviewer PDFkat0% (1)
- Topnotch Bridge Ob GyneDokument10 SeitenTopnotch Bridge Ob GyneAngela Saldajeno100% (1)
- Topnotch Mnemonics September 2016Dokument6 SeitenTopnotch Mnemonics September 2016Lian BaylosisNoch keine Bewertungen
- Blueprint For Questions Pharmacology and Therapeutics Subject Matter Question No. Recall Applica Tion Compre HensionDokument12 SeitenBlueprint For Questions Pharmacology and Therapeutics Subject Matter Question No. Recall Applica Tion Compre HensionJohn Christopher LucesNoch keine Bewertungen
- Topnotch Lab Interpretation For MoonlightersDokument41 SeitenTopnotch Lab Interpretation For Moonlightersmefav7778520Noch keine Bewertungen
- TTDokument101 SeitenTTralphNoch keine Bewertungen
- Pathology Supplement Handout Nov 2018Dokument25 SeitenPathology Supplement Handout Nov 2018Zak Kaz100% (2)
- Hi-Yield Notes in PCMDokument19 SeitenHi-Yield Notes in PCMJohn Christopher Luces100% (1)
- Suggested Review MaterialsDokument1 SeiteSuggested Review MaterialsJoher MendezNoch keine Bewertungen
- Philippine Physician Licensure Examination (Ple) : A Primer For Serviam by Exequiel Dimaano, MD WVSU COM Class 2013Dokument43 SeitenPhilippine Physician Licensure Examination (Ple) : A Primer For Serviam by Exequiel Dimaano, MD WVSU COM Class 2013Choi SpeaksNoch keine Bewertungen
- Suggested PLE ReviewersDokument1 SeiteSuggested PLE ReviewersBobet Reña80% (5)
- 1 Topnotch Biochemistry SuperExam1 PDFDokument92 Seiten1 Topnotch Biochemistry SuperExam1 PDFSheinna BarcelonaNoch keine Bewertungen
- TOPNOTCH Micro-Para Pearls September 2018 PDFDokument10 SeitenTOPNOTCH Micro-Para Pearls September 2018 PDFNica Lopez FernandezNoch keine Bewertungen
- Ple Sept 2019Dokument210 SeitenPle Sept 2019Zak Kaz86% (7)
- 06 - Topnotch Pathology SuperExam - NOHIGHLIGHTSDokument99 Seiten06 - Topnotch Pathology SuperExam - NOHIGHLIGHTSFrancine Lucas100% (1)
- PLE 2019 Preventive Medicine Answer KeyDokument7 SeitenPLE 2019 Preventive Medicine Answer Keydickson100% (1)
- Harrisons Reviewer Most Common 1Dokument59 SeitenHarrisons Reviewer Most Common 1Dre Valdez67% (3)
- Consent Prof SecrecyDokument27 SeitenConsent Prof Secrecy161 Syed Ali Turab ShahNoch keine Bewertungen
- 4 - Flores Vs PinedaDokument14 Seiten4 - Flores Vs Pinedamartina lopezNoch keine Bewertungen
- Medical and DeathcertificateDokument11 SeitenMedical and DeathcertificateRashmikaNoch keine Bewertungen
- Autism's Top 14 Areas of ConcernDokument2 SeitenAutism's Top 14 Areas of Concernmefav7778520Noch keine Bewertungen
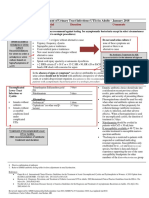
- Acute Gout ManagementDokument2 SeitenAcute Gout Managementmefav7778520Noch keine Bewertungen
- UTI Guideline Example 2 Appendix B PDFDokument4 SeitenUTI Guideline Example 2 Appendix B PDFamira catriNoch keine Bewertungen
- US Hypertension Review GuidelinesDokument12 SeitenUS Hypertension Review Guidelinesmefav7778520100% (1)
- Bell's Palsy: Diagnosis and ManagementDokument2 SeitenBell's Palsy: Diagnosis and Managementmefav7778520Noch keine Bewertungen
- Er Meds: DiclofenacDokument3 SeitenEr Meds: Diclofenacmefav7778520Noch keine Bewertungen
- Industrial HygieneDokument111 SeitenIndustrial Hygienemefav7778520100% (1)
- Basic Concept On Toxicology PDFDokument40 SeitenBasic Concept On Toxicology PDFmefav7778520Noch keine Bewertungen
- Compensation MedicineDokument46 SeitenCompensation Medicinemefav7778520Noch keine Bewertungen
- Drug Free WorkplaceDokument91 SeitenDrug Free Workplacemefav7778520Noch keine Bewertungen
- TB in The WorkplaceDokument60 SeitenTB in The Workplacemefav7778520100% (1)
- Do 53-03Dokument6 SeitenDo 53-03mefav7778520Noch keine Bewertungen
- Ococ Notes PDFDokument5 SeitenOcoc Notes PDFmefav7778520Noch keine Bewertungen
- 5s For SeptemberDokument17 Seiten5s For Septembermefav7778520Noch keine Bewertungen
- Topnotch Integrative MedicineDokument65 SeitenTopnotch Integrative Medicinemefav7778520Noch keine Bewertungen
- Accident CausationDokument104 SeitenAccident Causationmefav7778520Noch keine Bewertungen
- Side A - Forevermore PDFDokument5 SeitenSide A - Forevermore PDFmefav7778520100% (1)
- Topnotch IM For MoonlightersDokument274 SeitenTopnotch IM For Moonlightersmefav7778520100% (2)
- Pedia Notes Compilation MKDoseDokument18 SeitenPedia Notes Compilation MKDosemefav7778520Noch keine Bewertungen
- Topnotch Lab Interpretation For MoonlightersDokument41 SeitenTopnotch Lab Interpretation For Moonlightersmefav7778520Noch keine Bewertungen
- AAP Algorithm in Neonatal Hypoglycemia PDFDokument4 SeitenAAP Algorithm in Neonatal Hypoglycemia PDFmefav7778520Noch keine Bewertungen
- University of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - ConsortiumDokument17 SeitenUniversity of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - Consortiummefav7778520Noch keine Bewertungen
- AOM CPG RevisedDokument26 SeitenAOM CPG Revisedmefav7778520Noch keine Bewertungen
- Dengue Fever ReportDokument7 SeitenDengue Fever Reportmefav7778520Noch keine Bewertungen
- Multiple PregnancyDokument26 SeitenMultiple PregnancyOmar mohamedNoch keine Bewertungen
- Risk Factors Affecting PregnancyDokument6 SeitenRisk Factors Affecting PregnancyRoshin TejeroNoch keine Bewertungen
- Multifetal Pregnancy: Dr. Hani MahdiDokument59 SeitenMultifetal Pregnancy: Dr. Hani MahdiArwa QishtaNoch keine Bewertungen
- Riddles & Trick Questions For KidsDokument318 SeitenRiddles & Trick Questions For Kidsbaedaebok100% (3)
- Beta Met Has One Rcog GuidelineDokument9 SeitenBeta Met Has One Rcog GuidelineShefali MahindruNoch keine Bewertungen
- Multiple-Pregnancy - 2Dokument9 SeitenMultiple-Pregnancy - 2Queenie SilvaNoch keine Bewertungen
- The International Glossary On Infertility and Fertility Care, 2017Dokument14 SeitenThe International Glossary On Infertility and Fertility Care, 2017Zurya UdayanaNoch keine Bewertungen
- Provider Resources Obstetrics Late Preterm Steroids July2016Dokument10 SeitenProvider Resources Obstetrics Late Preterm Steroids July2016Pediatrics SLCM-WHQMNoch keine Bewertungen
- Acog Embarazo Gemelar 2004 PDFDokument15 SeitenAcog Embarazo Gemelar 2004 PDFEliel MarcanoNoch keine Bewertungen
- CPG Preterm Labor PDFDokument90 SeitenCPG Preterm Labor PDFJeffrey Arboleda100% (2)
- Placenta and Placental ProblemsDokument13 SeitenPlacenta and Placental ProblemsLuvita Ronteltap100% (1)
- Obstetric History & Examination SheetDokument8 SeitenObstetric History & Examination SheetVaibhav BhatiaNoch keine Bewertungen
- Constellation Close-Up: The Essential Guide To AstronomyDokument88 SeitenConstellation Close-Up: The Essential Guide To AstronomyStargateANoch keine Bewertungen
- Tachdjian's Pediatric Orthopaedics v.4Dokument660 SeitenTachdjian's Pediatric Orthopaedics v.4Leonardo Garay QuinteroNoch keine Bewertungen
- A (Certificate of Live Birth)Dokument3 SeitenA (Certificate of Live Birth)chate23100% (3)
- Maternal High-Dose DHA Supplementation and Neurodevelopment at 18-22 Months of Preterm ChildrenDokument10 SeitenMaternal High-Dose DHA Supplementation and Neurodevelopment at 18-22 Months of Preterm ChildrenEduardo Rios DuboisNoch keine Bewertungen
- Multiple Pregnancy NOR Poster PDFDokument1 SeiteMultiple Pregnancy NOR Poster PDFbigbossNoch keine Bewertungen
- Medley 2018Dokument67 SeitenMedley 2018Tú TúNoch keine Bewertungen
- Fit To Fly Expecting MotherDokument1 SeiteFit To Fly Expecting MotherAdnanAlamKhanNoch keine Bewertungen
- Multiple PregnancyDokument96 SeitenMultiple PregnancyNirmala PokharelNoch keine Bewertungen
- Guia Del Conocimiento CarnalDokument72 SeitenGuia Del Conocimiento CarnalVíctor Manuel Calatrava GallardoNoch keine Bewertungen
- Bayesian Analysis of Infant Mortality in Oyo State, NigeriaDokument6 SeitenBayesian Analysis of Infant Mortality in Oyo State, NigeriaInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Kehamilan GandaDokument18 SeitenKehamilan GandaLaris Donar Marukkap SihombingNoch keine Bewertungen
- VGO 421 ObstetricsDokument159 SeitenVGO 421 ObstetricsNaveen BasudeNoch keine Bewertungen
- Hs 130 Study Guide For Final AnswersDokument19 SeitenHs 130 Study Guide For Final AnswersHera Qureshi100% (1)
- In Vitro Fertilization (Ivf)Dokument2 SeitenIn Vitro Fertilization (Ivf)allfonsoNoch keine Bewertungen
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Dokument15 SeitenACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainNoch keine Bewertungen
- Causes of The UterineDokument7 SeitenCauses of The UterineDurgaValliNoch keine Bewertungen
- Shape It! SB 1Dokument13 SeitenShape It! SB 1Ass of Fire50% (6)
- Recent Advancement in Infertility Management and Adoption ProcessDokument161 SeitenRecent Advancement in Infertility Management and Adoption ProcessKripa Susan79% (24)