Das könnte Ihnen auch gefallen
- Alzheimer's Disease and Type 2 Diabetes Mellitus: Molecular Mechanisms and SimilaritiesDokument12 SeitenAlzheimer's Disease and Type 2 Diabetes Mellitus: Molecular Mechanisms and SimilaritiesMarco MerazNoch keine Bewertungen
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionVon EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNoch keine Bewertungen
- Pathophysiology of Cardiovascular Disease in Diabetes MellitusDokument6 SeitenPathophysiology of Cardiovascular Disease in Diabetes MellitusAnatomska CentralaNoch keine Bewertungen
- Research Paper On Diabetes Mellitus Type 2Dokument4 SeitenResearch Paper On Diabetes Mellitus Type 2gvzrg8jy100% (1)
- Pathogenesisof Cardiovasculardiseasein Diabetes: Andrea V. Haas,, Marie E. McdonnellDokument13 SeitenPathogenesisof Cardiovasculardiseasein Diabetes: Andrea V. Haas,, Marie E. McdonnellPaulina DiazNoch keine Bewertungen
- Metabolic Syndrome: Causes and Risks of Cluster of 5 ConditionsDokument119 SeitenMetabolic Syndrome: Causes and Risks of Cluster of 5 ConditionsMudassar SattarNoch keine Bewertungen
- Nutrition and Alzheimer's Disease risk reductionDokument8 SeitenNutrition and Alzheimer's Disease risk reductionPooja rameshNoch keine Bewertungen
- PPAR (Alpha) Its Role in The HDokument24 SeitenPPAR (Alpha) Its Role in The HGlagysDCarloNoch keine Bewertungen
- Haematological Parameters and Lipid Profile AbnormDokument10 SeitenHaematological Parameters and Lipid Profile AbnormPhelix O DaniyanNoch keine Bewertungen
- Oxidative Stress and Diabetes: Antioxidative StrategiesDokument18 SeitenOxidative Stress and Diabetes: Antioxidative StrategiesClaudia DoloresNoch keine Bewertungen
- Leptin and CKD MetabDokument16 SeitenLeptin and CKD MetabMita AdrianiNoch keine Bewertungen
- Literature Review On Diabetes Mellitus Type 2Dokument4 SeitenLiterature Review On Diabetes Mellitus Type 2qtbghsbnd100% (1)
- Role of Heme Oxygenase in Inflammation, Insulin-SignallingDokument18 SeitenRole of Heme Oxygenase in Inflammation, Insulin-SignallingAndri Praja SatriaNoch keine Bewertungen
- Non Alcoholic Fatty Liver Disease and Metabolic Syndrome: Invited ArticleDokument11 SeitenNon Alcoholic Fatty Liver Disease and Metabolic Syndrome: Invited ArticleBayu GemilangNoch keine Bewertungen
- Type 2 diabetes - managing blood sugar, diet, exercise and medicationsDokument10 SeitenType 2 diabetes - managing blood sugar, diet, exercise and medicationsExia QuinagonNoch keine Bewertungen
- Diabetes Mellitus Type 2 Research PaperDokument6 SeitenDiabetes Mellitus Type 2 Research Paperntjjkmrhf100% (1)
- Metabolic Syndrome - Wikipedia PDFDokument13 SeitenMetabolic Syndrome - Wikipedia PDFdeipodaNoch keine Bewertungen
- Current Concepts of Chronic Diabetic ComplicationsDokument4 SeitenCurrent Concepts of Chronic Diabetic ComplicationsscribdNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument15 SeitenNIH Public Access: Author ManuscriptIrma KurniawatiNoch keine Bewertungen
- Diabetes Dan HipertrofiDokument10 SeitenDiabetes Dan HipertrofiHanif FakhruddinNoch keine Bewertungen
- Type 2 Diabetes MellitusDokument24 SeitenType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (1)
- Diabetes LiteratureDokument6 SeitenDiabetes Literatureaba766467Noch keine Bewertungen
- Hyper Tension and Diabetes Mellitus: Gurushankar Govindarajan James R Sowers Craig S StumpDokument7 SeitenHyper Tension and Diabetes Mellitus: Gurushankar Govindarajan James R Sowers Craig S StumpAdina StoianNoch keine Bewertungen
- Type 2 Diabetes MellitusDokument19 SeitenType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Hindo Journal About Oxydative StressDokument25 SeitenHindo Journal About Oxydative StressBeddek AmiroucheNoch keine Bewertungen
- Srikant H 2016Dokument10 SeitenSrikant H 2016aditya sekarNoch keine Bewertungen
- Metabolic Syndrome as a Predictor of DiabetesDokument10 SeitenMetabolic Syndrome as a Predictor of DiabetesChiranjeeviNoch keine Bewertungen
- Epigenetics in The Development of Diabetic CardiomyopathyDokument4 SeitenEpigenetics in The Development of Diabetic CardiomyopathyJean Brando Torres GuerreroNoch keine Bewertungen
- Artigo 02Dokument18 SeitenArtigo 02Rozalia MedeirosNoch keine Bewertungen
- Accepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDokument30 SeitenAccepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsEster Elisabeth WoworNoch keine Bewertungen
- Ijms 24 09357 v2Dokument14 SeitenIjms 24 09357 v2MSNoch keine Bewertungen
- Nutrigenomics and cardiovascular gene regulationDokument6 SeitenNutrigenomics and cardiovascular gene regulationTrismegisteNoch keine Bewertungen
- CVD Effects of ExerciseDokument11 SeitenCVD Effects of ExerciseAboobacker SabithNoch keine Bewertungen
- Metabolic Syndrome: Learning ObjectivesDokument20 SeitenMetabolic Syndrome: Learning Objectivesddeeb420% (1)
- Nihms 1840957Dokument35 SeitenNihms 1840957Melda AngleNoch keine Bewertungen
- Marinedrugs 18 00357 v2Dokument20 SeitenMarinedrugs 18 00357 v2firman madao234Noch keine Bewertungen
- Endocrine Disrupting Chemicals Mediated Through Binding Androgen Receptor Are Associated With Diabetes MellitusDokument17 SeitenEndocrine Disrupting Chemicals Mediated Through Binding Androgen Receptor Are Associated With Diabetes MellitusDewi SartikaNoch keine Bewertungen
- Nutrients 13 00865Dokument11 SeitenNutrients 13 00865Roger CNoch keine Bewertungen
- Perspectives in Diabetes: Postprandial Hyperglycemia and Diabetes ComplicationsDokument7 SeitenPerspectives in Diabetes: Postprandial Hyperglycemia and Diabetes ComplicationsHania Asmarani RahmanitaNoch keine Bewertungen
- Literature Review On Type 2 Diabetes MellitusDokument7 SeitenLiterature Review On Type 2 Diabetes Mellituscmppcmwgf100% (1)
- Pathophysiology DM T2Dokument34 SeitenPathophysiology DM T2Andrea Duarte AriasNoch keine Bewertungen
- Diabetes Treatment Literature ReviewDokument7 SeitenDiabetes Treatment Literature Reviewafmzatvuipwdal100% (1)
- Zinc As A Potential Coadjuvant in Therapy For Type 2Dokument7 SeitenZinc As A Potential Coadjuvant in Therapy For Type 2Ida YulianaNoch keine Bewertungen
- Metabolic Syndrome and StrokeDokument5 SeitenMetabolic Syndrome and StrokeEmir SaricNoch keine Bewertungen
- Molecular Mechanisms of Obesity-Linked Cardiac DysDokument28 SeitenMolecular Mechanisms of Obesity-Linked Cardiac DysRebek EscutiaNoch keine Bewertungen
- Advances in Secondary Prevention Mechanisms of Macrovascular Complications in Type 2 Diabetes Mellitus Patients_ a Comprehensive Review. - Documento - Gale OneFile_ Nursing and Allied HealthDokument20 SeitenAdvances in Secondary Prevention Mechanisms of Macrovascular Complications in Type 2 Diabetes Mellitus Patients_ a Comprehensive Review. - Documento - Gale OneFile_ Nursing and Allied Healthabenavides39Noch keine Bewertungen
- Ban JASH2009Dokument15 SeitenBan JASH2009Adek FahmialdiNoch keine Bewertungen
- DM TyroidDokument10 SeitenDM TyroidKhuriyatun NadhifahNoch keine Bewertungen
- Oxidative Stress in The Cardiorenal Metabolic Syndrome: The Therapeutic Trials (G Mancia and TD Giles, Section Editors)Dokument6 SeitenOxidative Stress in The Cardiorenal Metabolic Syndrome: The Therapeutic Trials (G Mancia and TD Giles, Section Editors)filema2000Noch keine Bewertungen
- HHS Public Access: Autophagy in Diabetic Kidney Disease: Regulation, Pathological Role and Therapeutic PotentialDokument34 SeitenHHS Public Access: Autophagy in Diabetic Kidney Disease: Regulation, Pathological Role and Therapeutic PotentialdevyNoch keine Bewertungen
- Diabetes and Hyperlipidemia: A Direct Quantitative AnalysisDokument6 SeitenDiabetes and Hyperlipidemia: A Direct Quantitative AnalysisAnonymous Kc2tM8Noch keine Bewertungen
- Adiponectin and Alzheimer's Disease: Is There A Link?: ReviewDokument7 SeitenAdiponectin and Alzheimer's Disease: Is There A Link?: ReviewFritnerVélizNoch keine Bewertungen
- Concurrent TrainingDokument12 SeitenConcurrent Trainingfelipe diazNoch keine Bewertungen
- The Effects of Time-Released Garlic Powder Tablets On Multifunctional Cardiovascular Risk in Patients With Coronary Artery DiseaseDokument6 SeitenThe Effects of Time-Released Garlic Powder Tablets On Multifunctional Cardiovascular Risk in Patients With Coronary Artery DiseaseDayne LNoch keine Bewertungen
- Antioxidants: Plant Extracts For Type 2 Diabetes: From Traditional Medicine To Modern Drug DiscoveryDokument43 SeitenAntioxidants: Plant Extracts For Type 2 Diabetes: From Traditional Medicine To Modern Drug Discoverynur chasanahNoch keine Bewertungen
- Pathophysiology of Secondary Complications of Diabetes MellitusDokument6 SeitenPathophysiology of Secondary Complications of Diabetes MellitusWiler RgNoch keine Bewertungen
- Nutrients: Backstage of Eating Disorder-About The Biological Mechanisms Behind The Symptoms of Anorexia NervosaDokument32 SeitenNutrients: Backstage of Eating Disorder-About The Biological Mechanisms Behind The Symptoms of Anorexia NervosaMuh Rahmadan ANoch keine Bewertungen
- Protein oxidation in diabetes exploredDokument34 SeitenProtein oxidation in diabetes exploredAdelaKalstumAdiibahNoch keine Bewertungen
- Bio-Flavonoids With Promising Anti-Diabetic Potentials: A Critical SurveyDokument26 SeitenBio-Flavonoids With Promising Anti-Diabetic Potentials: A Critical SurveyKris Natalia ManihurukNoch keine Bewertungen
- LowBackPainDokument3 SeitenLowBackPainFATHICHAHNoch keine Bewertungen
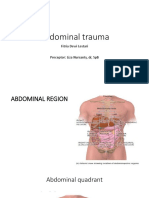
- CSS Abdominal Trauma PIPITDokument68 SeitenCSS Abdominal Trauma PIPITFATHICHAH0% (1)
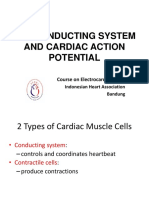
- 01-02. Ecg Course - The Conducting System and Cardiac Action PotentialDokument28 Seiten01-02. Ecg Course - The Conducting System and Cardiac Action PotentialFATHICHAHNoch keine Bewertungen
- CSS Hemoroid Bagian CahyaDokument41 SeitenCSS Hemoroid Bagian CahyaFATHICHAHNoch keine Bewertungen
- CSS - Suture Material & Suturing CabopoloDokument32 SeitenCSS - Suture Material & Suturing CabopoloFATHICHAHNoch keine Bewertungen
- Anes CSS 4Dokument5 SeitenAnes CSS 4FATHICHAHNoch keine Bewertungen
- CSS Hemoroid Bagian CahyaDokument41 SeitenCSS Hemoroid Bagian CahyaFATHICHAHNoch keine Bewertungen
- 01-02. Ecg Course - The Conducting System and Cardiac Action PotentialDokument28 Seiten01-02. Ecg Course - The Conducting System and Cardiac Action PotentialFATHICHAHNoch keine Bewertungen
- Growth Chart Dedi IrfanDokument40 SeitenGrowth Chart Dedi IrfanFATHICHAHNoch keine Bewertungen
- AlprazolamDokument2 SeitenAlprazolamFATHICHAHNoch keine Bewertungen
- AlprazolamDokument2 SeitenAlprazolamFATHICHAHNoch keine Bewertungen
- HEMOPHILIA GuidelinesDokument76 SeitenHEMOPHILIA Guidelinesmarco_jacinto1103197Noch keine Bewertungen
- Jadwal Rotasi - TA 2017-2018 - 19 September 2017Dokument7 SeitenJadwal Rotasi - TA 2017-2018 - 19 September 2017FATHICHAHNoch keine Bewertungen
- Jadwal Rotasi - TA 2017-2018 - 19 September 2017Dokument7 SeitenJadwal Rotasi - TA 2017-2018 - 19 September 2017FATHICHAHNoch keine Bewertungen
- 05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFDokument6 Seiten05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFrisda aulia putriNoch keine Bewertungen
- 1 - 07 - 220penatalaksanaan Medication-Overuse Headache PDFDokument5 Seiten1 - 07 - 220penatalaksanaan Medication-Overuse Headache PDFHeppyMei100% (1)
- Paraphrasing Summarising Lecture Exercises PDFDokument2 SeitenParaphrasing Summarising Lecture Exercises PDFDéboraChiaradia100% (1)
- The Research Paper: From Research Question To Final Draft A Scaffolded, 8-Week Program For Undergraduate StudentsDokument33 SeitenThe Research Paper: From Research Question To Final Draft A Scaffolded, 8-Week Program For Undergraduate StudentsRudyr BacolodNoch keine Bewertungen
- Subjective Global Assessment Form: Medical HistoryDokument2 SeitenSubjective Global Assessment Form: Medical Historynadia susiyanaNoch keine Bewertungen
- Food Chemistry: Andre Mu Ller, Hans SteinhartDokument9 SeitenFood Chemistry: Andre Mu Ller, Hans SteinhartAlfredo CruzNoch keine Bewertungen
- 18 Amazing Health Benefits From Honey and CinnamonDokument4 Seiten18 Amazing Health Benefits From Honey and Cinnamongladiola1100% (1)
- Anatomy ProjectDokument9 SeitenAnatomy Projectapi-391807326Noch keine Bewertungen
- BIOCHEMISTRY CARBOHYDRATESDokument100 SeitenBIOCHEMISTRY CARBOHYDRATESJiezl Abellano AfinidadNoch keine Bewertungen
- Heal Your Eye Problems With Herbs, Minerals and VitaminsDokument117 SeitenHeal Your Eye Problems With Herbs, Minerals and VitaminsAadilNoch keine Bewertungen
- Reading Comprehension Activity PDFDokument6 SeitenReading Comprehension Activity PDFSem KimNoch keine Bewertungen
- Dengue Discharge PlanDokument1 SeiteDengue Discharge PlanChris Denver BancaleNoch keine Bewertungen
- Nutrients, digestion, absorption and metabolism quizDokument12 SeitenNutrients, digestion, absorption and metabolism quizAnchal Singh100% (3)
- Brochure Physical ActivityDokument2 SeitenBrochure Physical Activityapi-340126515Noch keine Bewertungen
- Amosov ExercisesDokument3 SeitenAmosov Exercisesmladen1858948100% (1)
- CaffeineDokument31 SeitenCaffeinemaheshbabuhereNoch keine Bewertungen
- Shave 10 Hours Off Your WorkweekDokument50 SeitenShave 10 Hours Off Your WorkweekDimitri PetrovNoch keine Bewertungen
- Electrolyte and Acid Base EvaluationDokument78 SeitenElectrolyte and Acid Base EvaluationGiancarlo CajahuaringaNoch keine Bewertungen
- Antianemia Agents: Iron Vit B12 Folic Acid Copper Pyridoxine, RiboflavineDokument21 SeitenAntianemia Agents: Iron Vit B12 Folic Acid Copper Pyridoxine, RiboflavineRirin AfriantoNoch keine Bewertungen
- Physical Education Test ASJA Boys' College Charlieville Paper 2, Form 1, T3Dokument10 SeitenPhysical Education Test ASJA Boys' College Charlieville Paper 2, Form 1, T3asjawolverineNoch keine Bewertungen
- FD Buttbible 2018 EbookDokument155 SeitenFD Buttbible 2018 Ebooktuti100% (1)
- 90 Day Muscle Building Workout Plan Greatest Physiques PDFDokument12 Seiten90 Day Muscle Building Workout Plan Greatest Physiques PDFAli100% (1)
- Kerry Functional Health Benefits For Every GenerationDokument18 SeitenKerry Functional Health Benefits For Every GenerationNet SupraluckNoch keine Bewertungen
- Citrix MODokument6 SeitenCitrix MObilalmasNoch keine Bewertungen
- Nutrition Labeling Questions L1 Through L153: Guidance For Industry: A Food Labeling GuideDokument18 SeitenNutrition Labeling Questions L1 Through L153: Guidance For Industry: A Food Labeling GuidesrinuvoodiNoch keine Bewertungen
- Micro Niches You Can Work OnDokument6 SeitenMicro Niches You Can Work OnsaadNoch keine Bewertungen
- Health 7 Q2 Lasnutritional Needs of AdolescenceDokument17 SeitenHealth 7 Q2 Lasnutritional Needs of AdolescenceKathleen NacuaNoch keine Bewertungen
- 22 Highly-Effective Bar Exam Tips PDFDokument7 Seiten22 Highly-Effective Bar Exam Tips PDFMark Christian B. ApordoNoch keine Bewertungen
- 3 Azarpour Et Al. JNBR 4 (1) 2015 PDFDokument9 Seiten3 Azarpour Et Al. JNBR 4 (1) 2015 PDFKamailNoch keine Bewertungen
- Velez College - College of Nursing: F. Ramos ST., Cebu City S.Y. 2018 - 2019 Lesson PlanDokument5 SeitenVelez College - College of Nursing: F. Ramos ST., Cebu City S.Y. 2018 - 2019 Lesson Planinah krizia lagueNoch keine Bewertungen
- Mackenzie Martin ResumeDokument1 SeiteMackenzie Martin Resumeapi-294731342Noch keine Bewertungen
- Manage Chronic Kidney Disease and Its ComplicationsDokument35 SeitenManage Chronic Kidney Disease and Its ComplicationsTresnanda Bellawana100% (1)