Das könnte Ihnen auch gefallen
- Process Plant Layout - Seán Moran 3-4Dokument2 SeitenProcess Plant Layout - Seán Moran 3-4CunCunAlAndraNoch keine Bewertungen
- DA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DEDokument14 SeitenDA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DECunCunAlAndraNoch keine Bewertungen
- Process Plant Layout - Seán Moran 1-2Dokument2 SeitenProcess Plant Layout - Seán Moran 1-2CunCunAlAndra100% (1)
- GF Signet 515 2536 Manual01Dokument1 SeiteGF Signet 515 2536 Manual01CunCunAlAndraNoch keine Bewertungen
- Management Gathering 0718 - Distribution - v5 CoverDokument1 SeiteManagement Gathering 0718 - Distribution - v5 CoverCunCunAlAndraNoch keine Bewertungen
- Early Liver TransplantationDokument11 SeitenEarly Liver TransplantationCunCunAlAndraNoch keine Bewertungen
- Problem 5 Git: Ivan MichaelDokument68 SeitenProblem 5 Git: Ivan MichaelCunCunAlAndraNoch keine Bewertungen
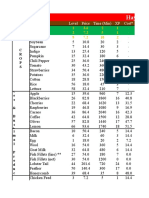
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisDokument154 SeitenPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraNoch keine Bewertungen
- RicoDokument62 SeitenRicoCunCunAlAndraNoch keine Bewertungen
- Breather Valve - Pressure-Vaccuem Relief ValveDokument2 SeitenBreather Valve - Pressure-Vaccuem Relief Valvevphor85Noch keine Bewertungen
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Gas Exchange & O2 TransportDokument11 SeitenGas Exchange & O2 Transportmina mounirNoch keine Bewertungen
- Lab 8Dokument6 SeitenLab 8Naz PulatNoch keine Bewertungen
- Obstructive Sleep ApneaDokument49 SeitenObstructive Sleep ApnearuthNoch keine Bewertungen
- Born To Snooze British English StudentDokument5 SeitenBorn To Snooze British English StudentislamNoch keine Bewertungen
- CH 10 BloodDokument65 SeitenCH 10 BloodAntonio Calleja IINoch keine Bewertungen
- GaltDokument5 SeitenGaltGlenn Kristie100% (1)
- Laporan Sel Darah Merah (Eritrosit)Dokument8 SeitenLaporan Sel Darah Merah (Eritrosit)RindiWirantikaNoch keine Bewertungen
- Introduction To Transfusion MedicineDokument12 SeitenIntroduction To Transfusion MedicineSamantha BuiNoch keine Bewertungen
- Summative Test in Science 6 Q2 W1-4Dokument1 SeiteSummative Test in Science 6 Q2 W1-4RHEA MARIE REYES100% (2)
- ImmunologyDokument3 SeitenImmunologybhawana bhattNoch keine Bewertungen
- Laju Digesti Pada Ikan FiksDokument12 SeitenLaju Digesti Pada Ikan FiksfataNoch keine Bewertungen
- Science 9 - First Quarter Reviewer: Biology 9Dokument33 SeitenScience 9 - First Quarter Reviewer: Biology 9Ace AligoraNoch keine Bewertungen
- Immunity: by Ashok K TiwariDokument42 SeitenImmunity: by Ashok K TiwariXEDGER09Noch keine Bewertungen
- THE GRASSHOPPERclassDokument37 SeitenTHE GRASSHOPPERclassSafiqa Tasfia100% (1)
- A. Strelnikova Breathing Exercises - Unique Method of Treating Chronic DiseasesDokument121 SeitenA. Strelnikova Breathing Exercises - Unique Method of Treating Chronic Diseaseslance wong100% (1)
- Alternate Overlap Syndrome 2023Dokument64 SeitenAlternate Overlap Syndrome 2023bonn maNoch keine Bewertungen
- Blood Group SystemsDokument7 SeitenBlood Group SystemshamaadaNoch keine Bewertungen
- The Digestive SystemDokument38 SeitenThe Digestive SystemrabiaNoch keine Bewertungen
- Daily Teaching PlanDokument3 SeitenDaily Teaching PlanOnie InoafNoch keine Bewertungen
- Atlas of Electroencephalography in Sleep MedicineDokument107 SeitenAtlas of Electroencephalography in Sleep MedicineReyna Luna-SaavedraNoch keine Bewertungen
- HB RespirationDokument6 SeitenHB RespirationJessicaWiryantoNoch keine Bewertungen
- Histology of Naval CavityDokument66 SeitenHistology of Naval CavityRomaine-Ricardo FrancisNoch keine Bewertungen
- Chapter-3 Movements and Breathing of Animals Subjective Question - AnswersDokument16 SeitenChapter-3 Movements and Breathing of Animals Subjective Question - AnswersabhinavNoch keine Bewertungen
- Topical Test 8 PDFDokument5 SeitenTopical Test 8 PDFHU LEE LEE MoeNoch keine Bewertungen
- Urinary SystemDokument7 SeitenUrinary SystemShelley CobbNoch keine Bewertungen
- Respiratory - Gas ExchangeDokument3 SeitenRespiratory - Gas ExchangeChris P. BeaconNoch keine Bewertungen
- Gambaran Elektrolit Serum Pada Anak Dengan Diare Akut PDFDokument6 SeitenGambaran Elektrolit Serum Pada Anak Dengan Diare Akut PDFCHRISTIN V.WOLOLI OBSGYN 22 juni - 26 juliNoch keine Bewertungen
- Anatomy and Physiology of Colon of Case StudyDokument4 SeitenAnatomy and Physiology of Colon of Case StudySimran JosanNoch keine Bewertungen
- A. Background: Truncus and Cauda. The Caput Part Is Relatively Small, Consist of A Beak Made FromDokument9 SeitenA. Background: Truncus and Cauda. The Caput Part Is Relatively Small, Consist of A Beak Made FromDaisy KavinskyNoch keine Bewertungen
- LP Grade 8Dokument1 SeiteLP Grade 8ayatolla ayatollaTMNoch keine Bewertungen