Das könnte Ihnen auch gefallen
- Shirvani 2013Dokument8 SeitenShirvani 2013santy27Noch keine Bewertungen
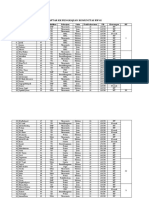
- Daftar KK Pengkajian Komunitas RW 02: Lampiran 6Dokument4 SeitenDaftar KK Pengkajian Komunitas RW 02: Lampiran 6santy27Noch keine Bewertungen
- Wjps 4 029Dokument7 SeitenWjps 4 029santy27Noch keine Bewertungen
- Ioi 140137Dokument9 SeitenIoi 140137santy27Noch keine Bewertungen
- S110 FullDokument10 SeitenS110 Fullsanty27Noch keine Bewertungen
- International Journal of Nursing Studies: M Isabel Rı Os-Risquez, Mariano Garcı A-IzquierdoDokument8 SeitenInternational Journal of Nursing Studies: M Isabel Rı Os-Risquez, Mariano Garcı A-Izquierdosanty27Noch keine Bewertungen
- Drury2013 PDFDokument9 SeitenDrury2013 PDFsanty27Noch keine Bewertungen
- Mortality Reduction For Fever, Hyperglycemia, and Swallowing Nurse-Initiated Stroke InterventionDokument7 SeitenMortality Reduction For Fever, Hyperglycemia, and Swallowing Nurse-Initiated Stroke Interventionsanty27Noch keine Bewertungen
- 10 1111@jog 12345Dokument7 Seiten10 1111@jog 12345santy27Noch keine Bewertungen
- Internet Video Chat Skype Family Conversations As A Treatment of Agitation in Nursing Home Residents With DementiaDokument2 SeitenInternet Video Chat Skype Family Conversations As A Treatment of Agitation in Nursing Home Residents With Dementiasanty27Noch keine Bewertungen
- SEPSIS KASUSDokument9 SeitenSEPSIS KASUSDilessandro PieroNoch keine Bewertungen
- Bingo There Was A Farmer Had A Dog and Bingo Was His Name-O B-I-N-G-O, B-I-N-G-O, B-I-N-G-O and Bingo Was His Name-ODokument1 SeiteBingo There Was A Farmer Had A Dog and Bingo Was His Name-O B-I-N-G-O, B-I-N-G-O, B-I-N-G-O and Bingo Was His Name-Osanty27Noch keine Bewertungen
- Innovative Collaborations Summary FINALDokument16 SeitenInnovative Collaborations Summary FINALsanty27Noch keine Bewertungen
- Secret MessageDokument2 SeitenSecret Messagesanty27Noch keine Bewertungen
- DiscoveryDokument1 SeiteDiscoverysanty27Noch keine Bewertungen
- Bits and Pieces in A TEYL Classroom - USD 2010Dokument24 SeitenBits and Pieces in A TEYL Classroom - USD 2010santy27Noch keine Bewertungen
- Perkembangan AnakDokument9 SeitenPerkembangan Anaksanty27Noch keine Bewertungen
- Community Nursing Diagnosis and PrioritizingDokument12 SeitenCommunity Nursing Diagnosis and Prioritizingsanty27Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Epidemiology of Diabetes MellitusDokument72 SeitenEpidemiology of Diabetes MellitusAnonymous RRkF0x67% (3)
- Chlamydia InfectionDokument5 SeitenChlamydia InfectionYogesh PhadtareNoch keine Bewertungen
- NCLEX Practice Exam For Pharmacology - Musculoskeletal Medications - RNpediaDokument8 SeitenNCLEX Practice Exam For Pharmacology - Musculoskeletal Medications - RNpediaKristine SingsonNoch keine Bewertungen
- Renal Exam Class TestDokument8 SeitenRenal Exam Class Test1fleetingNoch keine Bewertungen
- Bernabe Ncm109 LabDokument4 SeitenBernabe Ncm109 LabKarl LintanNoch keine Bewertungen
- Defining Treatment Response, Remission, Relapse, and RecoveryDokument21 SeitenDefining Treatment Response, Remission, Relapse, and Recovery주병욱Noch keine Bewertungen
- Emerging Re-Emerging Infectious Disease 2022Dokument57 SeitenEmerging Re-Emerging Infectious Disease 2022marioNoch keine Bewertungen
- APPROACH TO MANAGING JOINT PAINDokument44 SeitenAPPROACH TO MANAGING JOINT PAINKavya Anoop100% (1)
- C Post Concussion ChecklistDokument1 SeiteC Post Concussion Checklistalston96Noch keine Bewertungen
- Essay 5Dokument13 SeitenEssay 5api-549025764Noch keine Bewertungen
- Tnkhetp LBLDokument2 SeitenTnkhetp LBLvijayabhavani.sNoch keine Bewertungen
- Major Depressive Disorder in Adults: Diagnosis & Management: ScopeDokument19 SeitenMajor Depressive Disorder in Adults: Diagnosis & Management: ScopeBadii AmamouNoch keine Bewertungen
- Low-Level AutoimmunityDokument13 SeitenLow-Level AutoimmunityBeeBee SethNoch keine Bewertungen
- H&P Cheat SheetDokument3 SeitenH&P Cheat SheetWilliam YangNoch keine Bewertungen
- 7 Health Benefits of CoffeeDokument9 Seiten7 Health Benefits of CoffeeMaru PabloNoch keine Bewertungen
- Guideline Karsinoma HepatoselulerDokument11 SeitenGuideline Karsinoma HepatoselulerMohammad Ihsan RifasantoNoch keine Bewertungen
- Acute Myeloid LeukemiaDokument1 SeiteAcute Myeloid LeukemiaAlleah Salbo KepusNoch keine Bewertungen
- PERKENI (2021) - Konsensus DM Tipe 2Dokument119 SeitenPERKENI (2021) - Konsensus DM Tipe 2Ammalia RachmiNoch keine Bewertungen
- Esophagostomy Tube Complications in Dogs and CatsDokument6 SeitenEsophagostomy Tube Complications in Dogs and CatsDwi MahdaNoch keine Bewertungen
- Acute TonsillitisDokument54 SeitenAcute TonsillitissuciNoch keine Bewertungen
- Gold Standards in Medical FieldDokument8 SeitenGold Standards in Medical FieldJyothisankar Radhakrishnan100% (2)
- Medical Nutrition Therapy For Diseases of The MusculoskeletalDokument55 SeitenMedical Nutrition Therapy For Diseases of The MusculoskeletalSie ningsih100% (1)
- Psychiatrics McqsDokument20 SeitenPsychiatrics McqsHirwaNoch keine Bewertungen
- Public Warned vs. Chickenpox (Article From ABSCBN News) : ReflectionDokument1 SeitePublic Warned vs. Chickenpox (Article From ABSCBN News) : Reflectionkuu faalNoch keine Bewertungen
- Blood TransfusionDokument2 SeitenBlood TransfusionKomal TomarNoch keine Bewertungen
- Shan AsfDokument2 SeitenShan AsfM.Fizan JavedNoch keine Bewertungen
- Patient Anita NCPDokument15 SeitenPatient Anita NCPJoshoua MalanaNoch keine Bewertungen
- HSE Performance Statistics RecordDokument3 SeitenHSE Performance Statistics RecordGaneshNoch keine Bewertungen
- Camptodactyly: Amalia Irsha Adhari (1506668510) Eldesta Nisa Nabila (1406642233)Dokument38 SeitenCamptodactyly: Amalia Irsha Adhari (1506668510) Eldesta Nisa Nabila (1406642233)Amalia IrshaNoch keine Bewertungen
- NCP AidsDokument16 SeitenNCP AidstferdianingsihNoch keine Bewertungen