Das könnte Ihnen auch gefallen
- Van de Graaff GeneratorDokument10 SeitenVan de Graaff GeneratorJihad AnadNoch keine Bewertungen
- Uro SepsisDokument23 SeitenUro SepsisJihad Anad100% (1)
- Irrigating Fluids in Endoscopic Surgery: ReviewDokument12 SeitenIrrigating Fluids in Endoscopic Surgery: ReviewJihad AnadNoch keine Bewertungen
- Ultrasound NotesDokument19 SeitenUltrasound NotesJihad Anad100% (1)
- JSCFE Guidance Notes For Applicants - GenericDokument2 SeitenJSCFE Guidance Notes For Applicants - GenericJihad AnadNoch keine Bewertungen
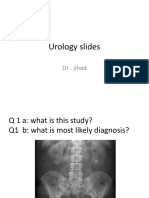
- Urology Slides: DR - JihadDokument4 SeitenUrology Slides: DR - JihadJihad Anad100% (1)
- Urology Slides: DR - JihadDokument4 SeitenUrology Slides: DR - JihadJihad Anad100% (1)
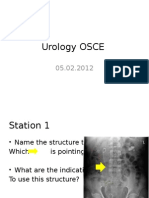
- Urology OSCEDokument9 SeitenUrology OSCEJihad Anad75% (4)
- JSCFE Guidance Notes For Referees - GenericDokument2 SeitenJSCFE Guidance Notes For Referees - GenericJihad AnadNoch keine Bewertungen
- Antibiotics: by Dr. Jihad AnadDokument89 SeitenAntibiotics: by Dr. Jihad AnadJihad AnadNoch keine Bewertungen
- DiureticsDokument6 SeitenDiureticsJihad AnadNoch keine Bewertungen
- Answer For Urology MCQDokument1 SeiteAnswer For Urology MCQJihad AnadNoch keine Bewertungen
- Aleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Dokument14 SeitenAleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Jihad AnadNoch keine Bewertungen
- Penile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceDokument4 SeitenPenile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceJihad AnadNoch keine Bewertungen
- ChoeDokument116 SeitenChoeJihad AnadNoch keine Bewertungen
- 500 Mcqs Surgery and RadiologyDokument66 Seiten500 Mcqs Surgery and RadiologyJihad Anad81% (59)
- ChoeDokument116 SeitenChoeJihad AnadNoch keine Bewertungen
- AbstractDokument2 SeitenAbstractJihad AnadNoch keine Bewertungen
- Success With Penile Prosthesis From Patient'S ViewpointDokument3 SeitenSuccess With Penile Prosthesis From Patient'S ViewpointJihad AnadNoch keine Bewertungen
- Appendix E: Microsoft Excel 2010 and Tools For Statistical AnalysisDokument15 SeitenAppendix E: Microsoft Excel 2010 and Tools For Statistical AnalysisJihad AnadNoch keine Bewertungen
- MCQ RadiologyDokument10 SeitenMCQ RadiologyJihad Anad100% (2)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Complete Blood Picture: Test Name Value Units Reference Range 3.44 7.4 76 22 28.5Dokument107 SeitenComplete Blood Picture: Test Name Value Units Reference Range 3.44 7.4 76 22 28.5anil tanankiNoch keine Bewertungen
- Preceptor PPT - HTMLDokument28 SeitenPreceptor PPT - HTMLwld_58hNoch keine Bewertungen
- Teratogens and Their EffectsDokument8 SeitenTeratogens and Their EffectsrayaimNoch keine Bewertungen
- Orahex Oral SolutionDokument1 SeiteOrahex Oral SolutionconanmarcNoch keine Bewertungen
- Abscess Case Pre FinalDokument41 SeitenAbscess Case Pre FinalDavid DueñasNoch keine Bewertungen
- CDC - Epidemiology and Prevention of Vaccine-Preventable DiseasesDokument458 SeitenCDC - Epidemiology and Prevention of Vaccine-Preventable DiseasesLewis Kim100% (1)
- Health Care Law OutlineDokument17 SeitenHealth Care Law OutlineMegan Lindsay Ruffin100% (1)
- Follicular LymphomaDokument12 SeitenFollicular LymphomaaymenNoch keine Bewertungen
- Total Gastrectomy ConsentDokument18 SeitenTotal Gastrectomy ConsentTanyaNganNoch keine Bewertungen
- CABGDokument14 SeitenCABGClaudette CayetanoNoch keine Bewertungen
- AKI7Dokument14 SeitenAKI7Kholida NabilaNoch keine Bewertungen
- Definition of Deviated Nasal SeptumDokument3 SeitenDefinition of Deviated Nasal SeptumMank BayuNoch keine Bewertungen
- Weight-Gain in Psychiatric TreatmentDokument19 SeitenWeight-Gain in Psychiatric Treatmentsvetlavb8063Noch keine Bewertungen
- Quick Reference Guide: Supported byDokument25 SeitenQuick Reference Guide: Supported byJanine HorsthNoch keine Bewertungen
- Introduction To Pharmacology AntibioticDokument15 SeitenIntroduction To Pharmacology AntibioticZaira Reine SantosNoch keine Bewertungen
- Ichroma II Test Panels 210331 104829Dokument2 SeitenIchroma II Test Panels 210331 104829Sinergy DiagnosticNoch keine Bewertungen
- Motion To DismissDokument16 SeitenMotion To DismissBasseemNoch keine Bewertungen
- Confidentiality in Pharmacy PracticeDokument20 SeitenConfidentiality in Pharmacy PracticeGeorge John AmegashieNoch keine Bewertungen
- Warfarin SodiumDokument3 SeitenWarfarin SodiumAndrea Huecas TriaNoch keine Bewertungen
- Abdominal TuberculosisDokument9 SeitenAbdominal TuberculosisImmanuelNoch keine Bewertungen
- Duties and Responsibilities of Allied Health PersonalDokument41 SeitenDuties and Responsibilities of Allied Health PersonalPushpinder Singh Sandhu100% (1)
- The Origins of The Clinical Pharmacy Program at UCSFDokument7 SeitenThe Origins of The Clinical Pharmacy Program at UCSFGerald GamboaNoch keine Bewertungen
- A Textbook of General Practice - 2nd EditionDokument336 SeitenA Textbook of General Practice - 2nd Editionstrahiltodorov100% (2)
- Highly Agressive Multiple Sclerosis PDFDokument26 SeitenHighly Agressive Multiple Sclerosis PDFnight.shadowNoch keine Bewertungen
- The Scoop On Brain Healt Dietary Supplement Products Containing Huperzine ADokument7 SeitenThe Scoop On Brain Healt Dietary Supplement Products Containing Huperzine Avasilyi IvanenkoNoch keine Bewertungen
- Essential Intra Natal Care 11aiDokument78 SeitenEssential Intra Natal Care 11aiDr Ankush VermaNoch keine Bewertungen
- Absorption of Drugs From Extravascular RoutesDokument11 SeitenAbsorption of Drugs From Extravascular RoutesraviNoch keine Bewertungen
- Manual Terapia DigitalDokument38 SeitenManual Terapia DigitalPaolaQuitian0% (1)
- Acute Renal FailureDokument34 SeitenAcute Renal Failureaibaloca67% (9)
- CABG Discharge Planning 1Dokument16 SeitenCABG Discharge Planning 1pipporudyNoch keine Bewertungen