Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Periapan Ujian MRCOG Fetal MedicineDokument224 SeitenPeriapan Ujian MRCOG Fetal MedicineAnnissa Syaira100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- AdenomyosisDokument4 SeitenAdenomyosisain trophisNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Ujian Lokal MCQDokument23 SeitenUjian Lokal MCQAnnissa Syaira100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Progesteron Friend or Foe ELSEVIERDokument15 SeitenProgesteron Friend or Foe ELSEVIERAnnissa SyairaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Ca CX in Pregnancy 2019 PDFDokument5 SeitenCa CX in Pregnancy 2019 PDFAnnissa SyairaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Slide DR - Relly Webinar POGI NTBDokument54 SeitenSlide DR - Relly Webinar POGI NTBAnnissa SyairaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Severe Covid-19: Clinical PracticeDokument10 SeitenSevere Covid-19: Clinical Practicemarcelocarvalhoteacher2373Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Management of Urinary Tract Infections in PregnancyDokument26 SeitenManagement of Urinary Tract Infections in PregnancySylvia WijayaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- ProQuestDocuments 2018 01 19Dokument26 SeitenProQuestDocuments 2018 01 19Annissa SyairaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Prolaps PanggulDokument5 SeitenProlaps Panggularina31Noch keine Bewertungen
- Calcineurin Signaling Mediates Activity-DependentDokument14 SeitenCalcineurin Signaling Mediates Activity-DependentAnnissa SyairaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Tocolytic Treatment in Pregnancy PDFDokument21 SeitenTocolytic Treatment in Pregnancy PDFLaiza JubyNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Calcineurin Signaling Mediates Activity-DependentDokument14 SeitenCalcineurin Signaling Mediates Activity-DependentAnnissa SyairaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Emerging Roles of The CalcineurinDokument33 SeitenEmerging Roles of The CalcineurinAnnissa SyairaNoch keine Bewertungen
- Onset and Persistence of Postpartum Depression in An Inner-City Maternal Health Clinic SystemDokument8 SeitenOnset and Persistence of Postpartum Depression in An Inner-City Maternal Health Clinic SystemAnnissa SyairaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- A Descriptive Model of Preventability in Maternal Morbidity and MortalityDokument6 SeitenA Descriptive Model of Preventability in Maternal Morbidity and MortalityAnnissa SyairaNoch keine Bewertungen
- s12884 014 0425 8Dokument17 Seitens12884 014 0425 8Annissa SyairaNoch keine Bewertungen
- DocumentDokument11 SeitenDocumentAnnissa SyairaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- 791 FullDokument7 Seiten791 FullAnnissa SyairaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Gambaran Histopatologi Plasenta Pada Kehamilan Dengan PreeklampsiaDokument6 SeitenGambaran Histopatologi Plasenta Pada Kehamilan Dengan PreeklampsiarobithaNoch keine Bewertungen
- A Descriptive Model of Preventability in Maternal Morbidity and MortalityDokument6 SeitenA Descriptive Model of Preventability in Maternal Morbidity and MortalityAnnissa SyairaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Research Report MScMed 11 May 2016Dokument79 SeitenResearch Report MScMed 11 May 2016Annissa SyairaNoch keine Bewertungen
- 1 PBDokument11 Seiten1 PBAnnissa SyairaNoch keine Bewertungen
- Pi Is 2352939317300155Dokument6 SeitenPi Is 2352939317300155Annissa SyairaNoch keine Bewertungen
- Ijpras 2016 5 3 326 334Dokument9 SeitenIjpras 2016 5 3 326 334rachel0301Noch keine Bewertungen
- Placental Growth Factor and Pre-Eclampsia: ReviewDokument5 SeitenPlacental Growth Factor and Pre-Eclampsia: ReviewAnnissa SyairaNoch keine Bewertungen
- Bai Tap Tieng Anh Lop 8 (Bai 13)Dokument4 SeitenBai Tap Tieng Anh Lop 8 (Bai 13)nguyenanhmaiNoch keine Bewertungen
- Reaction Paper-RprDokument6 SeitenReaction Paper-Rprapi-543457981Noch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Quality Factor of Inductor and CapacitorDokument4 SeitenQuality Factor of Inductor and CapacitoradimeghaNoch keine Bewertungen
- PPR Soft Copy Ayurvedic OkDokument168 SeitenPPR Soft Copy Ayurvedic OkKetan KathaneNoch keine Bewertungen
- Sav4747 PDFDokument49 SeitenSav4747 PDFAndres Antonio Moreno CastroNoch keine Bewertungen
- Pigeon Disease - The Eight Most Common Health Problems in PigeonsDokument2 SeitenPigeon Disease - The Eight Most Common Health Problems in Pigeonscc_lawrence100% (1)
- Inducement of Rapid Analysis For Determination of Reactive Silica and Available Alumina in BauxiteDokument11 SeitenInducement of Rapid Analysis For Determination of Reactive Silica and Available Alumina in BauxiteJAFAR MUHAMMADNoch keine Bewertungen
- Education in America: The Dumbing Down of The U.S. Education SystemDokument4 SeitenEducation in America: The Dumbing Down of The U.S. Education SystemmiichaanNoch keine Bewertungen
- AMS 48 - 2000-n - D0114354 - 055 - 00Dokument116 SeitenAMS 48 - 2000-n - D0114354 - 055 - 00wanhall100% (1)
- Chemistry Xi: Short Questions and 20% Long QuestionsDokument3 SeitenChemistry Xi: Short Questions and 20% Long QuestionsSyed Nabeel HassanNoch keine Bewertungen
- Class Two Summer Vacation AssignmentDokument1 SeiteClass Two Summer Vacation AssignmentshahbazjamNoch keine Bewertungen
- MajorProjects 202112 e 1Dokument64 SeitenMajorProjects 202112 e 1xtrooz abiNoch keine Bewertungen
- Report in Per Dev CorrectedDokument34 SeitenReport in Per Dev CorrectedJosh lyan RiveraNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- EP500 Standard Electropneumatic Positioner: Installation and Maintenance InstructionsDokument28 SeitenEP500 Standard Electropneumatic Positioner: Installation and Maintenance InstructionsAlan ValdezNoch keine Bewertungen
- Employee Final SettlementDokument1 SeiteEmployee Final SettlementZeeshan Mirza0% (1)
- A Project Report On A Study On Amul Taste of India: Vikash Degree College Sambalpur University, OdishaDokument32 SeitenA Project Report On A Study On Amul Taste of India: Vikash Degree College Sambalpur University, OdishaSonu PradhanNoch keine Bewertungen
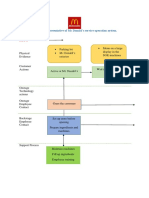
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDokument2 SeitenBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNoch keine Bewertungen
- Biochem Nucleic Acid ReviewerDokument5 SeitenBiochem Nucleic Acid ReviewerGabrielle FranciscoNoch keine Bewertungen
- Method StatementDokument29 SeitenMethod StatementZakwan Hisyam100% (1)
- ZJZJP Roots Vauum PumpDokument8 SeitenZJZJP Roots Vauum PumpAnonymous Tj3ApePIrNoch keine Bewertungen
- 5SDD 71B0210Dokument4 Seiten5SDD 71B0210Merter TolunNoch keine Bewertungen
- Big 9 Master SoalDokument6 SeitenBig 9 Master Soallilik masrukhahNoch keine Bewertungen
- Nitric AcidDokument7 SeitenNitric AcidKuldeep BhattNoch keine Bewertungen
- Cover Letter UchDokument1 SeiteCover Letter UchNakia nakia100% (1)
- 2133 Rla RlvaDokument2 Seiten2133 Rla RlvaAgung SubangunNoch keine Bewertungen
- Task 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Dokument5 SeitenTask 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Samir Mosquera-PalominoNoch keine Bewertungen
- DX340LC: Crawler ExcavatorDokument20 SeitenDX340LC: Crawler ExcavatorFeristha Meriani TabitaNoch keine Bewertungen
- Dr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFDokument72 SeitenDr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFagnesspratiwiNoch keine Bewertungen
- QA-QC TPL of Ecube LabDokument1 SeiteQA-QC TPL of Ecube LabManash Protim GogoiNoch keine Bewertungen
- Fast FashionDokument9 SeitenFast FashionTeresa GonzalezNoch keine Bewertungen
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayVon EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayBewertung: 4.5 von 5 Sternen4.5/5 (3)
- What to Expect When You’re Expecting (5th Edition)Von EverandWhat to Expect When You’re Expecting (5th Edition)Bewertung: 5 von 5 Sternen5/5 (1)
- Scaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Von EverandScaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Bewertung: 5 von 5 Sternen5/5 (1)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicVon EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNoch keine Bewertungen
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeVon EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeBewertung: 3.5 von 5 Sternen3.5/5 (13)
- The Five Dysfunctions of a Team SummaryVon EverandThe Five Dysfunctions of a Team SummaryBewertung: 4.5 von 5 Sternen4.5/5 (59)