Das könnte Ihnen auch gefallen
- HemiparesisDokument11 SeitenHemiparesisdindaNoch keine Bewertungen
- Ministry of Health and PopulationDokument1 SeiteMinistry of Health and PopulationDr Ahmed NabilNoch keine Bewertungen
- Pes Anserinus BursitisDokument6 SeitenPes Anserinus BursitisDr Ahmed NabilNoch keine Bewertungen
- Basu AP, Pearse J, Kelly S, Wisher V, Kisler J. - Frontiers in Neurology 2015, 5: 281Dokument10 SeitenBasu AP, Pearse J, Kelly S, Wisher V, Kisler J. - Frontiers in Neurology 2015, 5: 281Dr Ahmed NabilNoch keine Bewertungen
- Ministry of Health and PopulationDokument1 SeiteMinistry of Health and PopulationDr Ahmed NabilNoch keine Bewertungen
- ReviDokument7 SeitenReviDr Ahmed NabilNoch keine Bewertungen
- Blood Supply of The BrainDokument4 SeitenBlood Supply of The BrainDr Ahmed NabilNoch keine Bewertungen
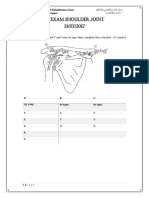
- 1st Exam Shoulder JointDokument5 Seiten1st Exam Shoulder JointDr Ahmed NabilNoch keine Bewertungen
- Revision On Anatomy of Cervical SpineDokument1 SeiteRevision On Anatomy of Cervical SpineDr Ahmed NabilNoch keine Bewertungen
- 8 Tips Worksheet 1Dokument1 Seite8 Tips Worksheet 1Dr Ahmed NabilNoch keine Bewertungen
- Key ActivitiesDokument1 SeiteKey ActivitiesDr Ahmed NabilNoch keine Bewertungen
- Avulsion Fracture of The Anterior Cruciate Ligament in A 9-Year-Old ChildDokument3 SeitenAvulsion Fracture of The Anterior Cruciate Ligament in A 9-Year-Old ChildDr Ahmed NabilNoch keine Bewertungen
- Therapeutic Programs For Musculoskeletal DisordersDokument1 SeiteTherapeutic Programs For Musculoskeletal DisordersDr Ahmed NabilNoch keine Bewertungen
- CE CertificateDokument1 SeiteCE CertificateDr Ahmed NabilNoch keine Bewertungen
- ADokument1 SeiteADr Ahmed NabilNoch keine Bewertungen
- Shoulder Assessment Patient Intake: Glenohumeral InstabilityDokument4 SeitenShoulder Assessment Patient Intake: Glenohumeral InstabilityDr Ahmed NabilNoch keine Bewertungen
- The 25 PROTOCOL: Important Exercise For SciaticaDokument8 SeitenThe 25 PROTOCOL: Important Exercise For SciaticaDr Ahmed NabilNoch keine Bewertungen
- Calories Mixed Dishes PDFDokument2 SeitenCalories Mixed Dishes PDFDr Ahmed NabilNoch keine Bewertungen
- السؤال الأولDokument1 Seiteالسؤال الأولDr Ahmed NabilNoch keine Bewertungen
- 1 Frozen ANEDokument7 Seiten1 Frozen ANEDr Ahmed NabilNoch keine Bewertungen
- Requirements For Licence by StateDokument20 SeitenRequirements For Licence by StatenehaNoch keine Bewertungen
- Section One: Hospital Overview: Departmental FunctionsDokument1 SeiteSection One: Hospital Overview: Departmental FunctionsDr Ahmed NabilNoch keine Bewertungen
- Therapeutic Programs For Musculoskeletal DisordersDokument1 SeiteTherapeutic Programs For Musculoskeletal DisordersDr Ahmed NabilNoch keine Bewertungen
- Physical Therapy GlossaryDokument3 SeitenPhysical Therapy GlossaryChristian BagoodNoch keine Bewertungen
- Lien 2000Dokument8 SeitenLien 2000Dr Ahmed NabilNoch keine Bewertungen
- Application DisabilityDokument7 SeitenApplication DisabilityMideauNoch keine Bewertungen
- To Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDokument7 SeitenTo Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDr Ahmed NabilNoch keine Bewertungen
- Dec Conform TBDokument1 SeiteDec Conform TBDr Ahmed NabilNoch keine Bewertungen
- Is There A Relation Between Shoulder Dysfunction and Core Instability?Dokument1 SeiteIs There A Relation Between Shoulder Dysfunction and Core Instability?Dr Ahmed NabilNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- SF36 Excel Score SheetDokument22 SeitenSF36 Excel Score SheetChoko DelgadoNoch keine Bewertungen
- Daftar Pustaka Frozen ShoulderDokument3 SeitenDaftar Pustaka Frozen ShoulderMuhammad Faza NaufalNoch keine Bewertungen
- Adhesive Capsulitis Presentation May 2009Dokument29 SeitenAdhesive Capsulitis Presentation May 2009cm4100% (1)
- Clinical Study: Effectiveness of Maitland Techniques in Idiopathic Shoulder Adhesive CapsulitisDokument9 SeitenClinical Study: Effectiveness of Maitland Techniques in Idiopathic Shoulder Adhesive CapsulitisAaron ChristhoperNoch keine Bewertungen
- Frozen...Dokument24 SeitenFrozen...Tutut RachmawatiNoch keine Bewertungen
- Shoulder Pain Diagnosis and Management in PrimaryDokument6 SeitenShoulder Pain Diagnosis and Management in PrimaryAnonymous ckZmIgoNoch keine Bewertungen
- Adhesive Capsulitis A Review of Current TreatmentDokument12 SeitenAdhesive Capsulitis A Review of Current TreatmentCamila Barrientos DíazNoch keine Bewertungen
- 13 - Daftar Pustaka NewDokument3 Seiten13 - Daftar Pustaka NewalfianiNoch keine Bewertungen
- Physical Therapy For Adhesive Capsulitis PDFDokument8 SeitenPhysical Therapy For Adhesive Capsulitis PDFАлексNoch keine Bewertungen
- Pathway For Shoulder PainDokument1 SeitePathway For Shoulder Painrizk86Noch keine Bewertungen
- Frozen Shoulder SummaryDokument8 SeitenFrozen Shoulder SummaryBobNoch keine Bewertungen
- Frozen Shoulder BookDokument85 SeitenFrozen Shoulder BookEdward Francis Seaton100% (2)
- Comparison of The Outcomes of Two Different Exercise Programs On Frozen ShoulderDokument8 SeitenComparison of The Outcomes of Two Different Exercise Programs On Frozen ShoulderbellaNoch keine Bewertungen
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategies For Frozen ShoulderDokument4 SeitenA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategies For Frozen ShoulderSergiNoch keine Bewertungen
- Evidence-Based Clinical Guidelines For The Diagnosis, Assessment and Physiotherapy Management of Contracted (Frozen) Shoulder: Quick ReferenceDokument4 SeitenEvidence-Based Clinical Guidelines For The Diagnosis, Assessment and Physiotherapy Management of Contracted (Frozen) Shoulder: Quick ReferenceDaniel DeinarovičNoch keine Bewertungen
- Exercise Frozen ShoulderDokument2 SeitenExercise Frozen ShoulderAnonymous D15WroNoch keine Bewertungen
- PT Ortho ProblemsDokument129 SeitenPT Ortho ProblemsvinaymanNoch keine Bewertungen
- The Surfers Shoulder PDFDokument24 SeitenThe Surfers Shoulder PDFSteveLangNoch keine Bewertungen
- Poster PapersDokument262 SeitenPoster PapersLeonardo RodríguezNoch keine Bewertungen
- Shoulder AnatomyDokument150 SeitenShoulder Anatomysrinidhi2011Noch keine Bewertungen
- Jurnal Frozen ShoulderDokument21 SeitenJurnal Frozen ShoulderMega Mulya Dwi FitriyaniNoch keine Bewertungen
- PT 2.2 2014 Student DossierDokument89 SeitenPT 2.2 2014 Student DossierArturo Ruiz LeónNoch keine Bewertungen
- Mama Points ExcerptDokument16 SeitenMama Points Excerptbromleydave100% (2)
- Hydrodilatation With Corticosteroid For The Treatment of Adhesive Capsulitis: A Systematic ReviewDokument13 SeitenHydrodilatation With Corticosteroid For The Treatment of Adhesive Capsulitis: A Systematic ReviewTesaTakwarifNoch keine Bewertungen
- Chronic Shoulder Pain - Part I Evaluation & DiagnosisDokument8 SeitenChronic Shoulder Pain - Part I Evaluation & Diagnosisgozjasa100% (1)
- Shoulder - Adhesive CapsulitisDokument9 SeitenShoulder - Adhesive Capsulitisvinayman100% (1)
- Shoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFDokument31 SeitenShoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFElliya RosyidaNoch keine Bewertungen
- Marma Points of Ayurveda Vasant Lad.09673Dokument18 SeitenMarma Points of Ayurveda Vasant Lad.09673Stephane Chollet75% (4)
- The Shoulder - Tung AcupointsDokument16 SeitenThe Shoulder - Tung Acupointspauloasv100% (3)
- Capsular Pattern Pada Idiopathic Frozen Shoulder: Oleh SugijantoDokument11 SeitenCapsular Pattern Pada Idiopathic Frozen Shoulder: Oleh SugijantoRhany JulyatiNoch keine Bewertungen