Das könnte Ihnen auch gefallen
- 4 Macabeos 1Dokument2 Seiten4 Macabeos 1Mafe SalazarNoch keine Bewertungen
- CriticalThinking Tutorial 1 PDFDokument3 SeitenCriticalThinking Tutorial 1 PDFMafe SalazarNoch keine Bewertungen
- SAM Fallacies1 PDFDokument9 SeitenSAM Fallacies1 PDFMaiyakabetaNoch keine Bewertungen
- Geometrical Solutions Derived From Mechanics - ArchimedesDokument28 SeitenGeometrical Solutions Derived From Mechanics - ArchimedesMafe SalazarNoch keine Bewertungen
- Critical Thinking in The Strong SenseDokument21 SeitenCritical Thinking in The Strong SenseMafe SalazarNoch keine Bewertungen
- Critical Thinking Template Analyzing The Logic of An ArticleDokument1 SeiteCritical Thinking Template Analyzing The Logic of An ArticleMafe SalazarNoch keine Bewertungen
- Hale Elements of ReasoningDokument53 SeitenHale Elements of ReasoningMafe SalazarNoch keine Bewertungen
- Logical ReasoningDokument595 SeitenLogical Reasoningynottrip100% (1)
- Critical ThinkingDokument16 SeitenCritical Thinkingal561471100% (1)
- Critical Thinking Planning QuestionsDokument1 SeiteCritical Thinking Planning QuestionsMafe SalazarNoch keine Bewertungen
- Critical Thinking and Reasoning Ch6 PDFDokument19 SeitenCritical Thinking and Reasoning Ch6 PDFMafe SalazarNoch keine Bewertungen
- Fallacies Poster 24 X 36Dokument1 SeiteFallacies Poster 24 X 36uuuttuuuNoch keine Bewertungen
- Critical Thinking For Everyday Life PDFDokument8 SeitenCritical Thinking For Everyday Life PDFMafe Salazar0% (1)
- Logic 1Dokument28 SeitenLogic 1polaris25Noch keine Bewertungen
- Dental Crowing and Its Relationship To Mesiodistal Crown Diameters and Arch DimensionsDokument7 SeitenDental Crowing and Its Relationship To Mesiodistal Crown Diameters and Arch DimensionsMafe SalazarNoch keine Bewertungen
- Age Changes of The Human Dental Arches by Multivariate TechniqueDokument9 SeitenAge Changes of The Human Dental Arches by Multivariate TechniqueMafe SalazarNoch keine Bewertungen
- Vancouver Condensed Guide 2015Dokument8 SeitenVancouver Condensed Guide 2015Sameer SharmaNoch keine Bewertungen
- Introducing Small Basic-1 PDFDokument69 SeitenIntroducing Small Basic-1 PDFnilaNoch keine Bewertungen
- Databases and Indexes For DentistryDokument6 SeitenDatabases and Indexes For DentistrynoxleekNoch keine Bewertungen
- Databases and Indexes For DentistryDokument6 SeitenDatabases and Indexes For DentistrynoxleekNoch keine Bewertungen
- Dental Arch Dimensions in Two Samples of Children 1950s and 1990sDokument7 SeitenDental Arch Dimensions in Two Samples of Children 1950s and 1990sMafe SalazarNoch keine Bewertungen
- Transverse Skeletal and Dentoalveolar Changes During Growth PDFDokument11 SeitenTransverse Skeletal and Dentoalveolar Changes During Growth PDFMafe SalazarNoch keine Bewertungen
- Developmental Changes of The Maxillary and Mandibular Dental Arches PDFDokument6 SeitenDevelopmental Changes of The Maxillary and Mandibular Dental Arches PDFMafe SalazarNoch keine Bewertungen
- International Association of Pediatric Dentistry - Children 0-2 Years of AgeDokument14 SeitenInternational Association of Pediatric Dentistry - Children 0-2 Years of AgeMafe SalazarNoch keine Bewertungen
- Pont S Index and Dental Arch FormDokument6 SeitenPont S Index and Dental Arch FormMafe SalazarNoch keine Bewertungen
- Changes in Dental Arch Dimensions Based On Biological AgeDokument13 SeitenChanges in Dental Arch Dimensions Based On Biological AgeMafe SalazarNoch keine Bewertungen
- Dental Arch Dimensions in Two Samples of Children 1950s and 1990sDokument7 SeitenDental Arch Dimensions in Two Samples of Children 1950s and 1990sMafe SalazarNoch keine Bewertungen
- Dental Arch Dimensions in Two Samples of Children 1950s and 1990sDokument7 SeitenDental Arch Dimensions in Two Samples of Children 1950s and 1990sMafe SalazarNoch keine Bewertungen
- Dental Arches in Various Etnic GroupsDokument7 SeitenDental Arches in Various Etnic GroupsMafe SalazarNoch keine Bewertungen
- Dental Arch Depth and Width Studied From 12 Years To AdulthoodDokument11 SeitenDental Arch Depth and Width Studied From 12 Years To AdulthoodMafe SalazarNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Cheat Sheet 2Dokument2 SeitenCheat Sheet 2oushaNoch keine Bewertungen
- Chapter 6 ProblemsDokument2 SeitenChapter 6 Problemswalt richardsNoch keine Bewertungen
- NeurosyphilisDokument8 SeitenNeurosyphilisl1o2stNoch keine Bewertungen
- Public Speaking ScriptDokument2 SeitenPublic Speaking Scriptsalbinarabi100% (1)
- Presentation of DiptheriaDokument45 SeitenPresentation of DiptheriaR-o-N-n-e-lNoch keine Bewertungen
- Nose Fracture and Deviated SeptumDokument17 SeitenNose Fracture and Deviated Septummimi2188Noch keine Bewertungen
- A Case of Subcorneal Pustular Dermatosis Successfully Treated With AcitretinDokument3 SeitenA Case of Subcorneal Pustular Dermatosis Successfully Treated With Acitretindr_RMNoch keine Bewertungen
- Cs Breast EngorgementDokument14 SeitenCs Breast Engorgementamit85% (13)
- Annatomy Notes For Bpe StudDokument14 SeitenAnnatomy Notes For Bpe StudYoga KalyanamNoch keine Bewertungen
- Appendectomy Surgery: What Is An Appendix?Dokument4 SeitenAppendectomy Surgery: What Is An Appendix?Muhammad Ichfan NabiuNoch keine Bewertungen
- Top 93 Nursing Skills, Procedures and Normal Values - OkDokument26 SeitenTop 93 Nursing Skills, Procedures and Normal Values - OkWilmaBongotanPadawil100% (1)
- Great Andamanese Lexicon EnglishDokument65 SeitenGreat Andamanese Lexicon EnglishSai VenkateshNoch keine Bewertungen
- Key Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !Dokument6 SeitenKey Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !June DumdumayaNoch keine Bewertungen
- A&P1 Final Exam Study GuideDokument7 SeitenA&P1 Final Exam Study GuideRhett ClarkNoch keine Bewertungen
- Tympanic MembraneDokument13 SeitenTympanic MembraneJerry NgNoch keine Bewertungen
- Physiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaDokument117 SeitenPhysiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaKithminaNoch keine Bewertungen
- Vitamin KDokument15 SeitenVitamin KTooba Sd100% (2)
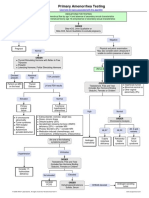
- Primary Amenorrhea Testing AlgorithmDokument1 SeitePrimary Amenorrhea Testing AlgorithmGabriella AguirreNoch keine Bewertungen
- Automated Cell Counts HB Estimation MethodsDokument10 SeitenAutomated Cell Counts HB Estimation Methodsjohn mwambuNoch keine Bewertungen
- Diseases, Ailments, and Disorders in Urinary System - PPTDokument24 SeitenDiseases, Ailments, and Disorders in Urinary System - PPTIsabella Alycia Lomibao100% (1)
- Charnley Ankle ArthrodesisDokument12 SeitenCharnley Ankle Arthrodesisdr_s_ganeshNoch keine Bewertungen
- Anatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterDokument75 SeitenAnatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterRuth AntolinNoch keine Bewertungen
- Minnesota State High School LeagueDokument2 SeitenMinnesota State High School Leagueapi-301794844Noch keine Bewertungen
- PEDOMAN Tatalaksana Cedera Otak 2014Dokument96 SeitenPEDOMAN Tatalaksana Cedera Otak 2014hasanNoch keine Bewertungen
- The Periodontal Ligament: A Unique, Multifunctional Connective TissueDokument21 SeitenThe Periodontal Ligament: A Unique, Multifunctional Connective TissueSamuel Flores CalderonNoch keine Bewertungen
- Child Immunization Record: Age in Months Nutrional StatusDokument14 SeitenChild Immunization Record: Age in Months Nutrional StatusMa. Jesica Salve LasundinNoch keine Bewertungen
- Breast Care in BreastfeedingDokument11 SeitenBreast Care in BreastfeedingBella Cy LopezNoch keine Bewertungen
- Talasemia de HB S y Talasemia de HB CDokument10 SeitenTalasemia de HB S y Talasemia de HB CAlejandra NúñezNoch keine Bewertungen
- Matilde-Tomaselli Cv-ShortDokument4 SeitenMatilde-Tomaselli Cv-Shortapi-308749490Noch keine Bewertungen
- ENGLISH GRAMMER For STD 6Dokument21 SeitenENGLISH GRAMMER For STD 6Joy OtanielNoch keine Bewertungen