Das könnte Ihnen auch gefallen
- Leopold' ManeuversDokument3 SeitenLeopold' Maneuversjava_biscocho122995% (22)
- Oncology Nursing Case StudyDokument16 SeitenOncology Nursing Case StudyJanJu J. Felizardo100% (1)
- IB Chemistry IA Eggshell LabDokument8 SeitenIB Chemistry IA Eggshell LabNour Makarem0% (3)
- 15 Exercises For Shoulder PainDokument2 Seiten15 Exercises For Shoulder PainMichael A FarinNoch keine Bewertungen
- GMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionVon EverandGMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionBewertung: 1 von 5 Sternen1/5 (1)
- Detoxification ProtocolsDokument231 SeitenDetoxification ProtocolsHanneke Thesame100% (6)
- Distal Radius Wrist Fracture Surgery Home Program Phase 2 Exercises PDFDokument4 SeitenDistal Radius Wrist Fracture Surgery Home Program Phase 2 Exercises PDFElizabeth ClarkNoch keine Bewertungen
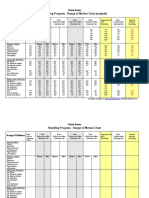
- Standing Program - Range of Motion Chart (Sample) : Client NameDokument2 SeitenStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNoch keine Bewertungen
- Bronson Card I A Rehab Home Exercise BookDokument31 SeitenBronson Card I A Rehab Home Exercise BookMariuca MaryNoch keine Bewertungen
- Ascorbic Acid ExperimentDokument10 SeitenAscorbic Acid ExperimentJoa YupNoch keine Bewertungen
- Prescribing Exercise For Adults - UpToDateDokument29 SeitenPrescribing Exercise For Adults - UpToDateAngga Julyananda PradanaNoch keine Bewertungen
- Exercise For Impaired BalanceDokument43 SeitenExercise For Impaired BalanceGildarts KunNoch keine Bewertungen
- Comprehensive Geriatric Assessment StudentDokument102 SeitenComprehensive Geriatric Assessment StudentCarelle Faith Serrano AsuncionNoch keine Bewertungen
- Chapter 04 - Rehabilitation Systems in Ambient Assisted Living EnvironmentsDokument19 SeitenChapter 04 - Rehabilitation Systems in Ambient Assisted Living EnvironmentsFernanda CamposNoch keine Bewertungen
- Manning Community Health Intro PageDokument4 SeitenManning Community Health Intro Pageapi-324335929Noch keine Bewertungen
- GRASP All 3 Levels11490 PDFDokument115 SeitenGRASP All 3 Levels11490 PDFAmit ZalaNoch keine Bewertungen
- Recommended Exercises For Different Age Groups and PeopleDokument8 SeitenRecommended Exercises For Different Age Groups and PeopleMawar Jingga0% (2)
- Pe and Health 11 Modules Week 1 and 2Dokument12 SeitenPe and Health 11 Modules Week 1 and 2RODJHEN ANNE P. BARQUILLANoch keine Bewertungen
- An 8 Week Scapular Stabilization Exercise Program in An Elite Archer With Scapular Dyskinesis Presenting Joint Noise A Case Report With One YearDokument8 SeitenAn 8 Week Scapular Stabilization Exercise Program in An Elite Archer With Scapular Dyskinesis Presenting Joint Noise A Case Report With One YearAmbrogio Orsini100% (1)
- 5th Lecture - Prevention & Control of Diseases - 12 Dec 2015Dokument41 Seiten5th Lecture - Prevention & Control of Diseases - 12 Dec 2015smbawasainiNoch keine Bewertungen
- Community Assessment FinalDokument16 SeitenCommunity Assessment Finalapi-311881661Noch keine Bewertungen
- B. Occupational Therapy (Hons.) : Faculty of Health Sciences Universiti Teknologi MaraDokument3 SeitenB. Occupational Therapy (Hons.) : Faculty of Health Sciences Universiti Teknologi MaraSiti Nur Hafidzoh OmarNoch keine Bewertungen
- HEP2GO Carpal Tunnel Program PDFDokument2 SeitenHEP2GO Carpal Tunnel Program PDFBetty OberackerNoch keine Bewertungen
- BKA ExercisesDokument8 SeitenBKA ExercisesMary Hope A. LimaNoch keine Bewertungen
- Range of Motion Exercises 2Dokument5 SeitenRange of Motion Exercises 2Attila TamasNoch keine Bewertungen
- Home HustleDokument4 SeitenHome Hustleapi-506702869Noch keine Bewertungen
- Cardiac RehabitationDokument4 SeitenCardiac Rehabitationsundar_kumar0Noch keine Bewertungen
- Wellness ProgramDokument14 SeitenWellness Programapi-383151067Noch keine Bewertungen
- Biases in Randomized Trials A Conversation Between Trialists and Epidemiologists.Dokument25 SeitenBiases in Randomized Trials A Conversation Between Trialists and Epidemiologists.Oscar Alexander Gutiérrez-LesmesNoch keine Bewertungen
- Introduction To Developmental Anatomy: Dr. Nitin VishwakarmaDokument78 SeitenIntroduction To Developmental Anatomy: Dr. Nitin Vishwakarmakissmyasthma69Noch keine Bewertungen
- Rehab Plans and Exercises Minor Rotator Cuff Repair Protocol For Physiotherapy Following SurgeryDokument11 SeitenRehab Plans and Exercises Minor Rotator Cuff Repair Protocol For Physiotherapy Following SurgeryTech How AssamNoch keine Bewertungen
- Range of Motion ExercisesDokument13 SeitenRange of Motion Exercisesmoira77Noch keine Bewertungen
- Glassgow Coma Scale and Rancho Los AmigosDokument17 SeitenGlassgow Coma Scale and Rancho Los AmigosHEMA CHANDRANNoch keine Bewertungen
- Jurnal Frozen ShoulderDokument21 SeitenJurnal Frozen ShoulderMega Mulya Dwi FitriyaniNoch keine Bewertungen
- Checklist - For - RANDOMIED CONTROLLED TRIALS PDFDokument9 SeitenChecklist - For - RANDOMIED CONTROLLED TRIALS PDFPIPE ELEJALDENoch keine Bewertungen
- USN Intro To FlexibilityDokument15 SeitenUSN Intro To FlexibilityJacobParkerNoch keine Bewertungen
- Sci RehabDokument45 SeitenSci RehabkaushikawebNoch keine Bewertungen
- Exercise Prescription Template s21-1Dokument5 SeitenExercise Prescription Template s21-1api-547397368Noch keine Bewertungen
- Exercise For Older AdultsDokument17 SeitenExercise For Older AdultsJawad AhmedNoch keine Bewertungen
- Effect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly PopulationDokument6 SeitenEffect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly Populationastrinila fauziNoch keine Bewertungen
- Home Exercise Program: Created by Namratha C Prabhu PT May 27th, 2015Dokument3 SeitenHome Exercise Program: Created by Namratha C Prabhu PT May 27th, 2015Ravindra Nadh Chowdary KammaNoch keine Bewertungen
- Using Physical Exercises To Improve Mental Health: SciencedirectDokument6 SeitenUsing Physical Exercises To Improve Mental Health: SciencedirectSry Lestari SamosirNoch keine Bewertungen
- Ballet GuidebookDokument36 SeitenBallet GuidebookAntonioAlvarezNoch keine Bewertungen
- YMCA Submaximal Cycle Test Worksheet Copy 2Dokument1 SeiteYMCA Submaximal Cycle Test Worksheet Copy 2Steve KandathilNoch keine Bewertungen
- 7-Minute Workout - Benefits, Intensity Level, and MoreDokument5 Seiten7-Minute Workout - Benefits, Intensity Level, and MoreFengNoch keine Bewertungen
- SCI Acute Care and Rehabilitation PT 2009Dokument265 SeitenSCI Acute Care and Rehabilitation PT 2009api-3822828Noch keine Bewertungen
- Tennis Elbow PDFDokument2 SeitenTennis Elbow PDFSabau PetreNoch keine Bewertungen
- Quiz 1: TestesDokument30 SeitenQuiz 1: TestesEmpress SaltNoch keine Bewertungen
- Cinahl Rotator Cuff InjuriesDokument11 SeitenCinahl Rotator Cuff InjurieslizardbeeNoch keine Bewertungen
- Human-Development-Part 2-Midwivery PDFDokument51 SeitenHuman-Development-Part 2-Midwivery PDFInselNoch keine Bewertungen
- Walking AidsDokument38 SeitenWalking AidsMurad KurdiNoch keine Bewertungen
- Range of Motion Exercises With PhotosDokument12 SeitenRange of Motion Exercises With PhotosSherly L WaromiNoch keine Bewertungen
- Getting Started: On Home OxygenDokument32 SeitenGetting Started: On Home OxygenJoyce TanNoch keine Bewertungen
- Theraex For IKFRDokument130 SeitenTheraex For IKFRsingle_ladyNoch keine Bewertungen
- Exercise Programs: Go ToDokument5 SeitenExercise Programs: Go Tojack sparrowNoch keine Bewertungen
- Development Chart For BookletDokument13 SeitenDevelopment Chart For BookletzapelNoch keine Bewertungen
- Joint, Connective Tissue, and Bone Disorders and ManagementDokument47 SeitenJoint, Connective Tissue, and Bone Disorders and ManagementAmbreen TariqNoch keine Bewertungen
- HMP (Hot Moist Pack W. Fluido Therapy)Dokument17 SeitenHMP (Hot Moist Pack W. Fluido Therapy)yamhtur_17100% (1)
- Home Exercise ProgramDokument6 SeitenHome Exercise ProgramRavin NarwalNoch keine Bewertungen
- Health Promotion Strategies For Stress ReductionDokument26 SeitenHealth Promotion Strategies For Stress Reductionezyl twotownNoch keine Bewertungen
- MGH Wrist and Elbow Strengthening ExercisesDokument1 SeiteMGH Wrist and Elbow Strengthening ExercisesRidwan Hadinata SalimNoch keine Bewertungen
- Anticipatory Guidance - The Older Adult 11-25-2017Dokument39 SeitenAnticipatory Guidance - The Older Adult 11-25-2017Abdul RohmanNoch keine Bewertungen
- Your Granny's Nurse: Your Guide to Aging and Compassionate Care for the ElderlyVon EverandYour Granny's Nurse: Your Guide to Aging and Compassionate Care for the ElderlyNoch keine Bewertungen
- Exercise your way to health: Arthritis: Exercise plans to improve your lifeVon EverandExercise your way to health: Arthritis: Exercise plans to improve your lifeNoch keine Bewertungen
- Scanned by CamscannerDokument22 SeitenScanned by CamscannerIreen PahangNoch keine Bewertungen
- MSK UsDokument32 SeitenMSK UsIreen PahangNoch keine Bewertungen
- 4886 65533 2 SP PDFDokument4 Seiten4886 65533 2 SP PDFIreen PahangNoch keine Bewertungen
- CPG PcapDokument25 SeitenCPG PcapIreen PahangNoch keine Bewertungen
- Tenebrio Molitor Meal in Rainbow Trout Oncorhynchus Mykiss Diets Effects On Animal Performance Nutrient Digestibility and Chemical Composition ofDokument8 SeitenTenebrio Molitor Meal in Rainbow Trout Oncorhynchus Mykiss Diets Effects On Animal Performance Nutrient Digestibility and Chemical Composition ofccbs2010Noch keine Bewertungen
- Formula Pakan KucingDokument22 SeitenFormula Pakan KucingShania100% (2)
- University of Cambridge International Examinations General Certificate of Education Ordinary LevelDokument16 SeitenUniversity of Cambridge International Examinations General Certificate of Education Ordinary Levelmstudy123456Noch keine Bewertungen
- Gestational Diabetes HandoutDokument2 SeitenGestational Diabetes Handoutapi-228263644Noch keine Bewertungen
- Anaemia in Pregnancy: Dr. Lama MehaisenDokument11 SeitenAnaemia in Pregnancy: Dr. Lama MehaisenWendy EvansNoch keine Bewertungen
- Microbiological Food HygieneDokument355 SeitenMicrobiological Food Hygieneogheeluv100% (3)
- Association Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenDokument6 SeitenAssociation Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenHarun joel tatipataNoch keine Bewertungen
- Design Thinking in Exercise - 27jan20Dokument18 SeitenDesign Thinking in Exercise - 27jan20ashlyn granthamNoch keine Bewertungen
- Ani Phy Ex 7Dokument4 SeitenAni Phy Ex 7YshaReyesNoch keine Bewertungen
- Al Fares Crown Spray Perfume IngredientDokument4 SeitenAl Fares Crown Spray Perfume IngredientSadruddin KamaruddinNoch keine Bewertungen
- Linear ProgrammingDokument18 SeitenLinear ProgrammingjebishaNoch keine Bewertungen
- Kevin Murphy PHD ThesisDokument5 SeitenKevin Murphy PHD Thesisnadinebenavidezfortworth100% (2)
- Diabetes: Statistics Symptoms Causes Diagnosis PreventionDokument67 SeitenDiabetes: Statistics Symptoms Causes Diagnosis PreventionShanthi_KVNoch keine Bewertungen
- Skin - Ayurveda and Modern ReferencesDokument3 SeitenSkin - Ayurveda and Modern Referencespadmaraj_pjNoch keine Bewertungen
- Ahara Vidhi: Concepts of Food Intake in Ayurveda With Comparison To Present EraDokument7 SeitenAhara Vidhi: Concepts of Food Intake in Ayurveda With Comparison To Present EraAjitānanda DāsaNoch keine Bewertungen
- The Carcass and Non-Carcass Parameters of Local Sheep Supplemented With Concentrate Mixture, Atella, Faidherbia Albida Leaf and Sesbania Sesban LeafDokument7 SeitenThe Carcass and Non-Carcass Parameters of Local Sheep Supplemented With Concentrate Mixture, Atella, Faidherbia Albida Leaf and Sesbania Sesban LeafFantahunNoch keine Bewertungen
- Neurogenic Bowel ManagementDokument51 SeitenNeurogenic Bowel ManagementAndrei TarusNoch keine Bewertungen
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationDokument2 SeitenNursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationCristoper BodionganNoch keine Bewertungen
- Kibble Shape and Its Effect On Feline PalatabilityDokument29 SeitenKibble Shape and Its Effect On Feline Palatabilitymutiara annisaaNoch keine Bewertungen
- Social Change Refers To An Alteration in The Social Order of A SocietyDokument4 SeitenSocial Change Refers To An Alteration in The Social Order of A SocietyAlan Valencia Baya Jr.Noch keine Bewertungen
- PetCo Iguana Care SheetDokument2 SeitenPetCo Iguana Care Sheetmicrosoft_userNoch keine Bewertungen
- What Is A Ketogenic Diet - The Beachbody BlogDokument10 SeitenWhat Is A Ketogenic Diet - The Beachbody BlogOni JotaNoch keine Bewertungen
- Pierderi K Si PDokument9 SeitenPierderi K Si PCristina Herman HanuschiNoch keine Bewertungen
- October 2012 Max MagazineDokument68 SeitenOctober 2012 Max MagazineMax Muscle San Mateo, CA & San Francisco (Castro), CANoch keine Bewertungen
- Module 1 NutritionLecDokument5 SeitenModule 1 NutritionLecbekbekk cabahugNoch keine Bewertungen