Das könnte Ihnen auch gefallen
- Barclays Money Skills Toolkit - Aged 16 - 25Dokument107 SeitenBarclays Money Skills Toolkit - Aged 16 - 25Josh BurkeNoch keine Bewertungen
- 24 Rudrajit EtalDokument6 Seiten24 Rudrajit EtaleditorijmrhsNoch keine Bewertungen
- Carvedilol and Nebivolol Improve Left Ventricular Systolic Functions in Patients With Non-Ischemic Heart FailureDokument6 SeitenCarvedilol and Nebivolol Improve Left Ventricular Systolic Functions in Patients With Non-Ischemic Heart FailureBramantyo DwiputraNoch keine Bewertungen
- Daniels Criteria - EKG in PEDokument10 SeitenDaniels Criteria - EKG in PEbrookswalsh100% (2)
- Pi Is 0894731703010198Dokument5 SeitenPi Is 0894731703010198Nag Mallesh RaoNoch keine Bewertungen
- The Type of The Functional Cardiovascular Response To Upright Posture Is Associated With Arterial Stiffness: A Cross-Sectional Study in 470 VolunteersDokument12 SeitenThe Type of The Functional Cardiovascular Response To Upright Posture Is Associated With Arterial Stiffness: A Cross-Sectional Study in 470 VolunteersVeNoch keine Bewertungen
- 228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Dokument2 Seiten228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Yulianty Saulina FransiscaNoch keine Bewertungen
- New 4Dokument11 SeitenNew 4abraham rumayaraNoch keine Bewertungen
- Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization EffectivenessDokument9 SeitenEvaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization EffectivenessMelisa AnaNoch keine Bewertungen
- 129 Full PDFDokument7 Seiten129 Full PDFHerlina ApriliaNoch keine Bewertungen
- Aawongece 2013Dokument8 SeitenAawongece 2013khan asifNoch keine Bewertungen
- SEHGAL 2016 - A New Look at Bronchopulmonary Dysplasia - Post Capillary Pathophysiology and Cardiac DysfunctionDokument8 SeitenSEHGAL 2016 - A New Look at Bronchopulmonary Dysplasia - Post Capillary Pathophysiology and Cardiac DysfunctionRafael JustinoNoch keine Bewertungen
- Clinical StudyDokument7 SeitenClinical StudyDian HasanahNoch keine Bewertungen
- Diagnostic and Prognostic Value of Plasma Volume Status at Emergency Department Admission in Dyspneic Patients Results From The PARADISE CohortDokument11 SeitenDiagnostic and Prognostic Value of Plasma Volume Status at Emergency Department Admission in Dyspneic Patients Results From The PARADISE CohortsunhaolanNoch keine Bewertungen
- 1405 9940 Acm 92 2 203Dokument6 Seiten1405 9940 Acm 92 2 203abdul alvarez ponceNoch keine Bewertungen
- BJAS-Volume 3-Issue 1 - Page 11-16Dokument6 SeitenBJAS-Volume 3-Issue 1 - Page 11-16rakaNoch keine Bewertungen
- BODEXDokument8 SeitenBODEXLindsey KaufmanNoch keine Bewertungen
- Clinical Research: Heart Failure/cardiomyopathyDokument11 SeitenClinical Research: Heart Failure/cardiomyopathyGustavo HenriqueNoch keine Bewertungen
- Sci 05 00034Dokument9 SeitenSci 05 00034aarthi devNoch keine Bewertungen
- Experimental Biology and MedicineDokument9 SeitenExperimental Biology and Medicineiri_balNoch keine Bewertungen
- Workload-Indexed Blood Pressure Response Is Superior To Peak Systolic Blood Pressure in Predicting All-Cause MortalityDokument10 SeitenWorkload-Indexed Blood Pressure Response Is Superior To Peak Systolic Blood Pressure in Predicting All-Cause MortalityEffendi UChinNoch keine Bewertungen
- 116 229 1 SMDokument6 Seiten116 229 1 SMsinlookerNoch keine Bewertungen
- European J of Heart Fail - 2006 - Cokkinos - Efficacy of Antithrombotic Therapy in Chronic Heart Failure The HELAS StudyDokument5 SeitenEuropean J of Heart Fail - 2006 - Cokkinos - Efficacy of Antithrombotic Therapy in Chronic Heart Failure The HELAS Studysebastián orejuelaNoch keine Bewertungen
- Moderate To Severe ASDokument7 SeitenModerate To Severe ASTheresia Sri RezekiNoch keine Bewertungen
- Summary and ConclusionDokument4 SeitenSummary and Conclusionhamodi222Noch keine Bewertungen
- Ajrccm 157 5 9709032Dokument5 SeitenAjrccm 157 5 9709032AlexandraGeorgeNoch keine Bewertungen
- Clinical Research: Heart Failure/cardiomyopathyDokument9 SeitenClinical Research: Heart Failure/cardiomyopathyAdam HuzaibyNoch keine Bewertungen
- Retired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialDokument9 SeitenRetired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialSarah GlennNoch keine Bewertungen
- Enhancing Detection Accuracy For Clinical Heart Failure Utilizing Pulse Transit Time Variability and Machine LearningDokument9 SeitenEnhancing Detection Accuracy For Clinical Heart Failure Utilizing Pulse Transit Time Variability and Machine LearningMuhammad SaimNoch keine Bewertungen
- Indian Journal of Nephrology Home: Download PDFDokument8 SeitenIndian Journal of Nephrology Home: Download PDFDr. Jatin GargNoch keine Bewertungen
- Bouremouth PresentationDokument10 SeitenBouremouth Presentationrhoda.aliu8888Noch keine Bewertungen
- J Geriatr Cardiol 2020 17 7 441-6Dokument6 SeitenJ Geriatr Cardiol 2020 17 7 441-6Fernando SousaNoch keine Bewertungen
- Eur J Echocardiogr 2007 Scardovi 30 6Dokument7 SeitenEur J Echocardiogr 2007 Scardovi 30 6Eman SadikNoch keine Bewertungen
- HFpEF Prevalence and Prognosis in COPD ExacerbationsDokument9 SeitenHFpEF Prevalence and Prognosis in COPD ExacerbationsFernandaNoch keine Bewertungen
- The University of Chicago Press Pulmonary Vascular Research InstituteDokument14 SeitenThe University of Chicago Press Pulmonary Vascular Research InstituteAmanda SmithNoch keine Bewertungen
- Assessment of Palpitation Complaints Benign Paroxysmal Positional VertigoDokument6 SeitenAssessment of Palpitation Complaints Benign Paroxysmal Positional VertigoHappy PramandaNoch keine Bewertungen
- Marchese 2019 Controlled Study of Central Hemodynamic ChangesDokument8 SeitenMarchese 2019 Controlled Study of Central Hemodynamic Changestaaaatan.04Noch keine Bewertungen
- Contoh Jurnal Meta AnalisisDokument17 SeitenContoh Jurnal Meta AnalisisMia Audina Miyanoshita100% (1)
- Okello2017 Article RheumaticHeartDiseaseInUgandaPDokument10 SeitenOkello2017 Article RheumaticHeartDiseaseInUgandaPyosefinNoch keine Bewertungen
- Emergency 1Dokument5 SeitenEmergency 1Liz LiwagNoch keine Bewertungen
- Chronic Kidney Disease and Statin Therapy: To Treat or Not To Treat?Dokument3 SeitenChronic Kidney Disease and Statin Therapy: To Treat or Not To Treat?adilNoch keine Bewertungen
- Decrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromeDokument7 SeitenDecrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromedarwigNoch keine Bewertungen
- Ioakeimidis2016Dokument9 SeitenIoakeimidis2016EnzoNoch keine Bewertungen
- Manuscript Mohamed TantawieyDokument13 SeitenManuscript Mohamed TantawieyMohamed TantawieyNoch keine Bewertungen
- Research ArticleDokument8 SeitenResearch ArticleMiguelNoch keine Bewertungen
- 10.1007@s10554 020 01913 6Dokument10 Seiten10.1007@s10554 020 01913 6Bosman AriestaNoch keine Bewertungen
- Atm 09 20 1587Dokument14 SeitenAtm 09 20 1587Wina Pertiwi 2003113414Noch keine Bewertungen
- Acute Respiratory Distress Syndrome (ARDS) - Associated Acute Cor Pulmonale and Patent Foramen Ovale: A Multicenter Noninvasive Hemodynamic StudyDokument6 SeitenAcute Respiratory Distress Syndrome (ARDS) - Associated Acute Cor Pulmonale and Patent Foramen Ovale: A Multicenter Noninvasive Hemodynamic StudyminiypuntoNoch keine Bewertungen
- Eci 12025Dokument11 SeitenEci 12025ger4ld1nNoch keine Bewertungen
- A Review of Heart Rate Variability and Its ApplicationsDokument6 SeitenA Review of Heart Rate Variability and Its ApplicationsBalkan RomeroNoch keine Bewertungen
- Meta-Analysis of Thoracic Epidural Anesthesia Versus General Anesthesia For Cardiac SurgeryDokument12 SeitenMeta-Analysis of Thoracic Epidural Anesthesia Versus General Anesthesia For Cardiac Surgery'-dooublleaiienn Itouehh IinNoch keine Bewertungen
- Thank GodDokument6 SeitenThank Godabraham rumayaraNoch keine Bewertungen
- Erythropoietin RequirementsDokument7 SeitenErythropoietin RequirementsMamad TrihatmowidjoyoNoch keine Bewertungen
- Atwater 2020Dokument6 SeitenAtwater 2020Vlada SiricNoch keine Bewertungen
- Jantung-Effect of L-Arginine On Cardiac Reverse Remodeling and Quality of Life inDokument8 SeitenJantung-Effect of L-Arginine On Cardiac Reverse Remodeling and Quality of Life inmerry christiantiNoch keine Bewertungen
- International Journal of Scientific Research: General MedicineDokument4 SeitenInternational Journal of Scientific Research: General MedicineTriple ANoch keine Bewertungen
- Dissert. AnisimovDokument7 SeitenDissert. AnisimovcamiloNoch keine Bewertungen
- C, B RecordDokument10 SeitenC, B RecordVjs MrunaliniNoch keine Bewertungen
- Research Paper Heart DiseaseDokument7 SeitenResearch Paper Heart Diseaseafeawfxlb100% (1)
- Prediction Clinical Profile To Distinguish Between Systolic and Diastolic Heart Failure in Hospitalized PatientsDokument6 SeitenPrediction Clinical Profile To Distinguish Between Systolic and Diastolic Heart Failure in Hospitalized PatientsVmiguel LcastilloNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyVon EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyBewertung: 1 von 5 Sternen1/5 (1)
- Neck LumpDokument18 SeitenNeck LumpJosh BurkeNoch keine Bewertungen
- Niel Gows Lament For The Death of His Second Wife-Mandolin-Tab PDFDokument1 SeiteNiel Gows Lament For The Death of His Second Wife-Mandolin-Tab PDFJosh BurkeNoch keine Bewertungen
- Central Nervous System Tumours OverviewDokument35 SeitenCentral Nervous System Tumours OverviewJosh BurkeNoch keine Bewertungen
- Antibiotics Study Guide 2017Dokument13 SeitenAntibiotics Study Guide 2017Josh BurkeNoch keine Bewertungen
- PoCUS Program 1016Dokument3 SeitenPoCUS Program 1016Josh BurkeNoch keine Bewertungen
- Hyponatraemia QuizDokument4 SeitenHyponatraemia QuizJosh BurkeNoch keine Bewertungen
- Block 5 Anatomy Seminar 1 Perineum MG - 5MAY2016Dokument22 SeitenBlock 5 Anatomy Seminar 1 Perineum MG - 5MAY2016Josh BurkeNoch keine Bewertungen
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDokument1 SeiteJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNoch keine Bewertungen
- IV Fluid Management: DR Andrew Stein Consultant Nephrologist, UHCWDokument37 SeitenIV Fluid Management: DR Andrew Stein Consultant Nephrologist, UHCWJosh BurkeNoch keine Bewertungen
- MurmursDokument2 SeitenMurmursJosh Burke100% (1)
- Abdo PainDokument35 SeitenAbdo PainJosh BurkeNoch keine Bewertungen
- Adult1 16-25 - 04sep16Dokument1 SeiteAdult1 16-25 - 04sep16Josh BurkeNoch keine Bewertungen
- Physiology of Pregnancy - Pre-Eclampsia DiabetesDokument34 SeitenPhysiology of Pregnancy - Pre-Eclampsia DiabetesJosh BurkeNoch keine Bewertungen
- Blood Sugars - DiabetesDokument31 SeitenBlood Sugars - DiabetesJosh BurkeNoch keine Bewertungen
- Physical Exam Reasons: Hands, Eyes, and MoreDokument1 SeitePhysical Exam Reasons: Hands, Eyes, and MoreJosh BurkeNoch keine Bewertungen
- Professional Behaviour and Fitness To Practise 0816.PDF 66085925Dokument84 SeitenProfessional Behaviour and Fitness To Practise 0816.PDF 66085925Josh BurkeNoch keine Bewertungen
- Anxiety and Panic Attacks: Symptoms and Risk FactorsDokument11 SeitenAnxiety and Panic Attacks: Symptoms and Risk FactorsJosh BurkeNoch keine Bewertungen
- R IntroDokument105 SeitenR Introtp2006sterNoch keine Bewertungen
- Symptoms and Risk FactorsDokument4 SeitenSymptoms and Risk FactorsJosh BurkeNoch keine Bewertungen
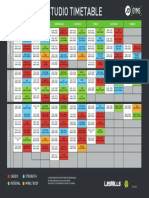
- Coventry Timetable SEP16Dokument1 SeiteCoventry Timetable SEP16Josh BurkeNoch keine Bewertungen
- R IntroDokument105 SeitenR Introtp2006sterNoch keine Bewertungen
- Handel HWV348 50hha - Violin1Dokument13 SeitenHandel HWV348 50hha - Violin1Josh BurkeNoch keine Bewertungen
- Leclair 6 Sonatas Op.3 Nos 4 6Dokument25 SeitenLeclair 6 Sonatas Op.3 Nos 4 6Josh Burke100% (2)
- Beriot Method Part 1Dokument78 SeitenBeriot Method Part 1Caitriona HollandNoch keine Bewertungen
- Bruni 6 Duettini Op.34Dokument24 SeitenBruni 6 Duettini Op.34Josh BurkeNoch keine Bewertungen
- Softship SeabearDokument1 SeiteSoftship SeabearJosh BurkeNoch keine Bewertungen
- Crockpot RecipiesDokument45 SeitenCrockpot RecipiescpantsulaNoch keine Bewertungen
- Heartjnl 2019 314702 Inline Supplementary Material 2Dokument3 SeitenHeartjnl 2019 314702 Inline Supplementary Material 2البكالوريوس المكثف فى التمريضNoch keine Bewertungen
- Group 1 - Cardiorespiratory Exercise ProgramDokument32 SeitenGroup 1 - Cardiorespiratory Exercise ProgramSmiley Jhen Garcia SabinianoNoch keine Bewertungen
- Samson Notes 2014Dokument345 SeitenSamson Notes 2014Hamza Ahmed100% (1)
- MRI Case Study Cervical SpineDokument15 SeitenMRI Case Study Cervical SpineTunas HarapanNoch keine Bewertungen
- 2020 Focused Transesophageal Echocardiography During Cardiac Arrest ResuscitationDokument10 Seiten2020 Focused Transesophageal Echocardiography During Cardiac Arrest Resuscitationbogeg74816Noch keine Bewertungen
- Drug Study - DigoxinDokument2 SeitenDrug Study - DigoxinKian Herrera50% (2)
- Choosing the Right Cardiac Stress TestDokument75 SeitenChoosing the Right Cardiac Stress TestLakshmi PrasannaNoch keine Bewertungen
- Phys9 06 1Dokument6 SeitenPhys9 06 1alifia azzahraNoch keine Bewertungen
- The Heart Is Not A Pump - The Blood Moves The Heart, Not Vice VersaDokument14 SeitenThe Heart Is Not A Pump - The Blood Moves The Heart, Not Vice VersagiovacaneNoch keine Bewertungen
- Pulmonary EmbolismDokument3 SeitenPulmonary EmbolismdeanneadrianoNoch keine Bewertungen
- 2 Quarter 1 Module 2 CirculatoryDokument21 Seiten2 Quarter 1 Module 2 CirculatoryJasmine Paz0% (1)
- AHA 2017 Cardiogenic ShockDokument37 SeitenAHA 2017 Cardiogenic ShockAnastasyaLianNoch keine Bewertungen
- Week 2 Circulatory SystemDokument7 SeitenWeek 2 Circulatory SystemCarl Brian L. MonteverdeNoch keine Bewertungen
- CARDIOLOGY TIPSDokument53 SeitenCARDIOLOGY TIPSPangalanitaNoch keine Bewertungen
- Heart Disease Thesis StatementDokument6 SeitenHeart Disease Thesis StatementHelpWithPaperCanada100% (2)
- Refractory AnginaDokument19 SeitenRefractory AnginaVijay KumarNoch keine Bewertungen
- The Egyptian Heart Journal: Ahmed Elshazly, Hazem Khorshid, Hany Hanna, Ammar AliDokument3 SeitenThe Egyptian Heart Journal: Ahmed Elshazly, Hazem Khorshid, Hany Hanna, Ammar AliImran TarmiziNoch keine Bewertungen
- Blood Vessels CH 13Dokument86 SeitenBlood Vessels CH 13Nalla Mirelle CarbonellNoch keine Bewertungen
- Lab-3 Toads Heart Contractile ResponseDokument4 SeitenLab-3 Toads Heart Contractile ResponseWilson CheungNoch keine Bewertungen
- NMS Surgery Casebook CH 1 Preoperative Care Flashcards - ProProfsDokument3 SeitenNMS Surgery Casebook CH 1 Preoperative Care Flashcards - ProProfsWade Bullock0% (1)
- High Blood PressureDokument9 SeitenHigh Blood PressureshashidharanNoch keine Bewertungen
- Current Use and Advances in Vasopressors and Inotropes Support in ShockDokument13 SeitenCurrent Use and Advances in Vasopressors and Inotropes Support in ShockJose Luis Espino MacielNoch keine Bewertungen
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDokument4 SeitenKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNoch keine Bewertungen
- Normal BP Girls - UpToDate PDFDokument3 SeitenNormal BP Girls - UpToDate PDFcharoite100% (1)
- CVP MonitoringDokument36 SeitenCVP MonitoringFlorence SanchezNoch keine Bewertungen
- Scientech 2351: FeaturesDokument2 SeitenScientech 2351: FeaturesSudip KunduNoch keine Bewertungen
- Septum Formation in The VentriclesDokument43 SeitenSeptum Formation in The VentriclesAhsan IslamNoch keine Bewertungen
- Activity 1 - Effect of Blood Vessel Radius On Blood Flow Rate PDFDokument5 SeitenActivity 1 - Effect of Blood Vessel Radius On Blood Flow Rate PDFTadhg Ó MaoldhomhnaighNoch keine Bewertungen
- Management Arteriosclerosis and ClaudicationDokument41 SeitenManagement Arteriosclerosis and ClaudicationLuqman AlwiNoch keine Bewertungen
- Pagewriter Xli Users GuideDokument129 SeitenPagewriter Xli Users Guidemebme2022Noch keine Bewertungen