Das könnte Ihnen auch gefallen
- NANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESVon EverandNANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESNoch keine Bewertungen
- Recent Advances in Novel Drug Delivery SystemsDokument11 SeitenRecent Advances in Novel Drug Delivery SystemsNico GiménezNoch keine Bewertungen
- Liquid Membranes: Principles and Applications in Chemical Separations and Wastewater TreatmentVon EverandLiquid Membranes: Principles and Applications in Chemical Separations and Wastewater TreatmentNoch keine Bewertungen
- Dheeraj Project Final PDFDokument28 SeitenDheeraj Project Final PDFDrAmit Verma100% (1)
- Noble Drug Delivery System Project Report For LrietDokument25 SeitenNoble Drug Delivery System Project Report For LrietAshish NavalNoch keine Bewertungen
- Drug Delevery SystemDokument15 SeitenDrug Delevery SystempravincrNoch keine Bewertungen
- Final Project 29-04-2010Dokument38 SeitenFinal Project 29-04-2010DRx Anuj ChauhanNoch keine Bewertungen
- Microsphere: A Review: IJRPC 2011, 1Dokument15 SeitenMicrosphere: A Review: IJRPC 2011, 1Mahendra ReddyNoch keine Bewertungen
- Nanocarriers Dendrimers: Targeted Drug DeliveryDokument15 SeitenNanocarriers Dendrimers: Targeted Drug DeliverychandrakantpatelNoch keine Bewertungen
- Drug Delivery Systems: Nanoparticles, Microspheres and LiposomesDokument6 SeitenDrug Delivery Systems: Nanoparticles, Microspheres and LiposomesANoch keine Bewertungen
- Niosomes As Nano-Delivery Systems in The Pharmaceutical FieldDokument18 SeitenNiosomes As Nano-Delivery Systems in The Pharmaceutical FieldLuciana BetzlerNoch keine Bewertungen
- Hyjek_Jodlowski_Metal-organic_2_2023Dokument72 SeitenHyjek_Jodlowski_Metal-organic_2_2023zeinab bakhodaNoch keine Bewertungen
- Bioceramics and Pharmaceuticals A Remarkable SynergyDokument9 SeitenBioceramics and Pharmaceuticals A Remarkable Synergycollin samuelNoch keine Bewertungen
- Mucoadhesive Multiparticulate Drug Delivery Systems: An Extensive Review of PatentsDokument18 SeitenMucoadhesive Multiparticulate Drug Delivery Systems: An Extensive Review of PatentsIndri AuraliaNoch keine Bewertungen
- Polymer Nanoparticles For Smart Drug Delivery: Devasier Bennet and Sanghyo KimDokument54 SeitenPolymer Nanoparticles For Smart Drug Delivery: Devasier Bennet and Sanghyo KimMonica TurnerNoch keine Bewertungen
- Drug DeliveryDokument17 SeitenDrug DeliveryHinal AmbasanaNoch keine Bewertungen
- Novel Mucoadhesive Polymers - A Review: Mythri .G, K. Kavitha, M. Rupesh Kumar, Sd. Jagadeesh SinghDokument6 SeitenNovel Mucoadhesive Polymers - A Review: Mythri .G, K. Kavitha, M. Rupesh Kumar, Sd. Jagadeesh SinghRajesh KumarNoch keine Bewertungen
- Out PDFDokument6 SeitenOut PDFDafne CarolinaNoch keine Bewertungen
- 26 CMC PDFDokument10 Seiten26 CMC PDF8612106535Noch keine Bewertungen
- Silica particles deliver drugsDokument8 SeitenSilica particles deliver drugsNitesh JajuNoch keine Bewertungen
- Drug Delivery System in Bone Regeneration and Implant DentistryDokument29 SeitenDrug Delivery System in Bone Regeneration and Implant DentistrySilvia SoareNoch keine Bewertungen
- Surface Modification Techniques For Active Targeting of Polymeric NanoparticlesDokument20 SeitenSurface Modification Techniques For Active Targeting of Polymeric NanoparticlesInternational Journal of Pharma Bioscience and Technology (ISSN: 2321-2969)Noch keine Bewertungen
- Microencapsulation As A Novel Drug Delivery System: Vol. 1 - Issue 1 - ©2011 IPSDokument7 SeitenMicroencapsulation As A Novel Drug Delivery System: Vol. 1 - Issue 1 - ©2011 IPSsameersyed77Noch keine Bewertungen
- Microencapsulation A Promising Technique For ContrDokument13 SeitenMicroencapsulation A Promising Technique For ContrPhúc NguyễnNoch keine Bewertungen
- Topical Drug DeliveryDokument21 SeitenTopical Drug DeliveryhappyNoch keine Bewertungen
- IntroductionDokument27 SeitenIntroductionSanjeevKumarNoch keine Bewertungen
- Pharmaceutics 14 00359 v2Dokument37 SeitenPharmaceutics 14 00359 v2Dominik EwaldNoch keine Bewertungen
- Chitosan nanoparticles for drug deliveryDokument17 SeitenChitosan nanoparticles for drug deliveryUMY HABIBANoch keine Bewertungen
- Ajptr 102021 111Dokument16 SeitenAjptr 102021 11188-pranjal VasavNoch keine Bewertungen
- 5 645465024025853986 PDFDokument17 Seiten5 645465024025853986 PDFAnonymous ZwkjFokJNCNoch keine Bewertungen
- Concepts of Buccal Drug Delivery System: Bioadhesion and MucoadhesionDokument6 SeitenConcepts of Buccal Drug Delivery System: Bioadhesion and Mucoadhesionpathuri rangaNoch keine Bewertungen
- Mucoadhesive Microencapsulation: A New Tool in Drug Delivery SystemsDokument61 SeitenMucoadhesive Microencapsulation: A New Tool in Drug Delivery SystemsLailatul QadarNoch keine Bewertungen
- Polymeric Nanoparticles For Drug Delivery Recent D PDFDokument41 SeitenPolymeric Nanoparticles For Drug Delivery Recent D PDFNguyễn HiềnNoch keine Bewertungen
- Polymers, Polymers, EverywhereDokument7 SeitenPolymers, Polymers, EverywhereKausik Singh ThakurNoch keine Bewertungen
- Jurnal 1Dokument22 SeitenJurnal 1RuwindaNoch keine Bewertungen
- 1.1. Nanotechnology: Nanotechnology Is The Science and Technology at Nano Scale, Which Ranges About 1-100Dokument22 Seiten1.1. Nanotechnology: Nanotechnology Is The Science and Technology at Nano Scale, Which Ranges About 1-100Subham BoseNoch keine Bewertungen
- Micro CapsulationDokument28 SeitenMicro CapsulationArun AhirwarNoch keine Bewertungen
- The Involvement of The Mitochondrial Membrane in Drug DeliveryDokument69 SeitenThe Involvement of The Mitochondrial Membrane in Drug Deliveryf.tellelopezNoch keine Bewertungen
- Multi Particulate Drug Delivery SystemDokument23 SeitenMulti Particulate Drug Delivery Systemasifghasi100% (1)
- Designing Hydrogels For ControlledDokument17 SeitenDesigning Hydrogels For ControlledJohn AcostaNoch keine Bewertungen
- Microspheres - An Overview: Prasanth V.V, Akash Chakraborthy Moy, Sam T Mathew, Rinku MathapanDokument7 SeitenMicrospheres - An Overview: Prasanth V.V, Akash Chakraborthy Moy, Sam T Mathew, Rinku MathapanMadhu Mohan Paudel ChettriNoch keine Bewertungen
- Mechanism of Implantable Drug Delivery SystemsDokument48 SeitenMechanism of Implantable Drug Delivery SystemsTanveer AhmedNoch keine Bewertungen
- Expert Review Poly (Ethylene Glycol) - Modified Nanocarriers For Tumor-Targeted and Intracellular DeliveryDokument10 SeitenExpert Review Poly (Ethylene Glycol) - Modified Nanocarriers For Tumor-Targeted and Intracellular Deliverym_ssNoch keine Bewertungen
- CN StevanovicDokument15 SeitenCN StevanovicMonica TurnerNoch keine Bewertungen
- NTC 6150 NanoBiotechnology Unit 5 2022-23Dokument52 SeitenNTC 6150 NanoBiotechnology Unit 5 2022-23Ayush DubeyNoch keine Bewertungen
- Targeted Nanocarriers for Cancer TherapyDokument20 SeitenTargeted Nanocarriers for Cancer Therapyalex_andra_22Noch keine Bewertungen
- Resumen Segundo Corte.Dokument19 SeitenResumen Segundo Corte.NELLYS ENITH MOGROBEJO ALVAREZ ESTUDIANTE ACTIVONoch keine Bewertungen
- A Prolonged Release Parenteral Drug Delivery SystemDokument11 SeitenA Prolonged Release Parenteral Drug Delivery SystemronnymcmNoch keine Bewertungen
- Formulation and Evaluation of Floating Microspheres of Metformin HydrochlorideDokument10 SeitenFormulation and Evaluation of Floating Microspheres of Metformin HydrochlorideBaru Chandrasekhar RaoNoch keine Bewertungen
- Bme 401-5Dokument15 SeitenBme 401-5Emmanuel NwankwoNoch keine Bewertungen
- Review ArticleDokument9 SeitenReview ArticlemickydivyaNoch keine Bewertungen
- Polymers 12 02825 v2Dokument38 SeitenPolymers 12 02825 v2pratikshaNoch keine Bewertungen
- Oral Delivery of Macromolecular DrugsDokument11 SeitenOral Delivery of Macromolecular DrugsharrisshoaibNoch keine Bewertungen
- 1.Microsponges Review Article (1) (1)Dokument12 Seiten1.Microsponges Review Article (1) (1)Ana VlasceanuNoch keine Bewertungen
- Bio Nano PartDokument14 SeitenBio Nano Partomoy43Noch keine Bewertungen
- Polymer in Drug DeliveryDokument42 SeitenPolymer in Drug DeliverysaudNoch keine Bewertungen
- Protein Nanoparticle: A Unique System As Drug Delivery VehiclesDokument9 SeitenProtein Nanoparticle: A Unique System As Drug Delivery VehiclesAndrei PrecupNoch keine Bewertungen
- Paper 8Dokument23 SeitenPaper 8cbrs.vetmedNoch keine Bewertungen
- Nano Biotechnology FinalDokument16 SeitenNano Biotechnology FinalMinhaj Haider100% (3)
- 4614183Dokument13 Seiten4614183Andreea MicuNoch keine Bewertungen
- Content 9080Dokument7 SeitenContent 9080Andreea MicuNoch keine Bewertungen
- 2.modulation of Adipogenic Conditions For Prospective Use ofDokument20 Seiten2.modulation of Adipogenic Conditions For Prospective Use ofAndreea MicuNoch keine Bewertungen
- Stem Cells Down Under ISSCR 2007 2007 Cell Stem CellDokument6 SeitenStem Cells Down Under ISSCR 2007 2007 Cell Stem CellAndreea MicuNoch keine Bewertungen
- Characterization and Comparison of Mesoporous Silica Particles For Optimized Drug DeliveryDokument15 SeitenCharacterization and Comparison of Mesoporous Silica Particles For Optimized Drug DeliveryAndreea MicuNoch keine Bewertungen
- 0pancreatic Cancer Stem Cells and Therapeutic Approaches!!!!!!Dokument15 Seiten0pancreatic Cancer Stem Cells and Therapeutic Approaches!!!!!!Andreea MicuNoch keine Bewertungen
- 43-049... Sandeep Kumar... Review... Plants... 220-228Dokument13 Seiten43-049... Sandeep Kumar... Review... Plants... 220-228Andreea MicuNoch keine Bewertungen
- Expression of Survivin, A Novel Inhibitor of Apoptosis and Cell Cycle Regulatory Protein, in Pancreatic AdenocarcinomaDokument7 SeitenExpression of Survivin, A Novel Inhibitor of Apoptosis and Cell Cycle Regulatory Protein, in Pancreatic AdenocarcinomaAndreea MicuNoch keine Bewertungen
- Identification of Pancreatic Cancer Stem CellsDokument9 SeitenIdentification of Pancreatic Cancer Stem CellsAndreea MicuNoch keine Bewertungen
- Identification of Pancreatic Cancer Stem CellsDokument9 SeitenIdentification of Pancreatic Cancer Stem CellsAndreea MicuNoch keine Bewertungen
- Iovanna Şi Colab., 2012 PDFDokument24 SeitenIovanna Şi Colab., 2012 PDFAndreea MicuNoch keine Bewertungen
- Riding A BikeDokument8 SeitenRiding A BikeAndreea MicuNoch keine Bewertungen
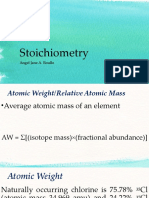
- Stoichiometry: Angel Jane A. RoulloDokument39 SeitenStoichiometry: Angel Jane A. RoulloLoren EsguerraNoch keine Bewertungen
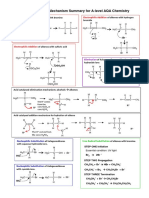
- Aqa Mechanisms A Level SummaryDokument5 SeitenAqa Mechanisms A Level SummaryRS JNoch keine Bewertungen
- Lower Yatta District Form Four Evaluation Test Chemistry Paper 3 Marking SchemeDokument3 SeitenLower Yatta District Form Four Evaluation Test Chemistry Paper 3 Marking SchemeKaroki Francis KagombeNoch keine Bewertungen
- Brochure Syngas ClariantDokument9 SeitenBrochure Syngas ClariantDiego Plana RobertNoch keine Bewertungen
- ISO 17025 NDT Lab Accreditation CertificateDokument3 SeitenISO 17025 NDT Lab Accreditation Certificatekiki270977Noch keine Bewertungen
- Determine nutrients with lab testsDokument5 SeitenDetermine nutrients with lab testsDevi RambaranNoch keine Bewertungen
- 11.3 Relative Stability of Element Group 14Dokument13 Seiten11.3 Relative Stability of Element Group 14吴绍轩Noch keine Bewertungen
- Use of N2 Gas For Purging in GTAW of SSDokument4 SeitenUse of N2 Gas For Purging in GTAW of SSrondulf goNoch keine Bewertungen
- Lipid nanoparticles may serve as glue between metals and nucleic acidsDokument8 SeitenLipid nanoparticles may serve as glue between metals and nucleic acidsÓscar SánchezNoch keine Bewertungen
- European Patent Application C07F 7/08: Method For Preparation of Organohydrogen PolysiloxanesDokument5 SeitenEuropean Patent Application C07F 7/08: Method For Preparation of Organohydrogen Polysiloxanesswaroop_exlncNoch keine Bewertungen
- 6C. AntioxidantsDokument2 Seiten6C. AntioxidantsKim Xiarisse BalugayNoch keine Bewertungen
- Phenol: Carboxylation of Phenol: Kolb-Schmitt ReactionDokument9 SeitenPhenol: Carboxylation of Phenol: Kolb-Schmitt ReactionAkhilaNoch keine Bewertungen
- Assignment-5 Enmt610029 Welding ANDARADHI NARARYA/1206291992Dokument8 SeitenAssignment-5 Enmt610029 Welding ANDARADHI NARARYA/1206291992Andaradhi NararyaNoch keine Bewertungen
- Effects of Silicon Surfactant in Rigid Polyurethane FoamsDokument7 SeitenEffects of Silicon Surfactant in Rigid Polyurethane Foamsธนพล กัตติยบุตรNoch keine Bewertungen
- Specification Data: Starquick® Self-Locking Pipe ClampDokument6 SeitenSpecification Data: Starquick® Self-Locking Pipe ClampأبومحمدالزياتNoch keine Bewertungen
- Skin Creams: Revision)Dokument13 SeitenSkin Creams: Revision)SaraNoch keine Bewertungen
- The Composition of Exhaust Gases From Diesel Gasoline and Propane Powered Motor CoachesDokument7 SeitenThe Composition of Exhaust Gases From Diesel Gasoline and Propane Powered Motor CoachesAhmad BilaalNoch keine Bewertungen
- Dissolvine GL Technical BrochureDokument13 SeitenDissolvine GL Technical BrochurealejandroNoch keine Bewertungen
- Mott - HyPulse Element FilterDokument12 SeitenMott - HyPulse Element FilterCristhian CuevaNoch keine Bewertungen
- A Study On Spinel Formation PDFDokument5 SeitenA Study On Spinel Formation PDFBagas Prasetyawan Adi NugrohoNoch keine Bewertungen
- Lithium Metaborate: Libo Formula WT 49.75 CAS No. 13453-69-5Dokument4 SeitenLithium Metaborate: Libo Formula WT 49.75 CAS No. 13453-69-5jycortesNoch keine Bewertungen
- 1.7 Batch Cell Culture 2Dokument36 Seiten1.7 Batch Cell Culture 2Astra BeckettNoch keine Bewertungen
- Chloride: Silver Nitrate Method Method 8207 10 To 10,000 MG/L As CL Digital TitratorDokument6 SeitenChloride: Silver Nitrate Method Method 8207 10 To 10,000 MG/L As CL Digital TitratorAlbertoNoch keine Bewertungen
- How to Prevent Sulfate Attack on ConcreteDokument19 SeitenHow to Prevent Sulfate Attack on ConcreteIrvebry Ayu WulandaryNoch keine Bewertungen
- Power-to-Steel Study: Steel-Making Systems To Reduce CO Emissions by Utilizing Renewable Energy in The German Steel IndustryDokument10 SeitenPower-to-Steel Study: Steel-Making Systems To Reduce CO Emissions by Utilizing Renewable Energy in The German Steel IndustryEvira Bella YustianiNoch keine Bewertungen
- Straw FiltersDokument9 SeitenStraw Filtersapi-340815123Noch keine Bewertungen
- 2 - ArrowPushingDokument14 Seiten2 - ArrowPushingYoung GothNoch keine Bewertungen
- Engineering materials properties guideDokument5 SeitenEngineering materials properties guideRam SwaroopNoch keine Bewertungen
- Specification For: Anodic Oxide Coatings On Wrought Aluminium For External Architectural ApplicationsDokument19 SeitenSpecification For: Anodic Oxide Coatings On Wrought Aluminium For External Architectural ApplicationschandimadissanayakaNoch keine Bewertungen
- Formula 1955 Organic Hand CreamDokument1 SeiteFormula 1955 Organic Hand CreamSafiullah KhanNoch keine Bewertungen
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsVon EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNoch keine Bewertungen
- Guidelines for Chemical Process Quantitative Risk AnalysisVon EverandGuidelines for Chemical Process Quantitative Risk AnalysisBewertung: 5 von 5 Sternen5/5 (1)
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksVon EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksBewertung: 5 von 5 Sternen5/5 (1)
- Guidelines for the Management of Change for Process SafetyVon EverandGuidelines for the Management of Change for Process SafetyNoch keine Bewertungen
- Piping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationVon EverandPiping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationBewertung: 4 von 5 Sternen4/5 (18)
- Nuclear Energy in the 21st Century: World Nuclear University PressVon EverandNuclear Energy in the 21st Century: World Nuclear University PressBewertung: 4.5 von 5 Sternen4.5/5 (3)
- Trevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationVon EverandTrevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationNoch keine Bewertungen
- Produced Water Treatment Field ManualVon EverandProduced Water Treatment Field ManualBewertung: 4.5 von 5 Sternen4.5/5 (5)
- Guidelines for Siting and Layout of FacilitiesVon EverandGuidelines for Siting and Layout of FacilitiesNoch keine Bewertungen
- Process Engineering for a Small Planet: How to Reuse, Re-Purpose, and Retrofit Existing Process EquipmentVon EverandProcess Engineering for a Small Planet: How to Reuse, Re-Purpose, and Retrofit Existing Process EquipmentNoch keine Bewertungen
- Well Control for Completions and InterventionsVon EverandWell Control for Completions and InterventionsBewertung: 4 von 5 Sternen4/5 (10)
- Guidelines for Vapor Cloud Explosion, Pressure Vessel Burst, BLEVE, and Flash Fire HazardsVon EverandGuidelines for Vapor Cloud Explosion, Pressure Vessel Burst, BLEVE, and Flash Fire HazardsNoch keine Bewertungen
- Guidelines for Enabling Conditions and Conditional Modifiers in Layer of Protection AnalysisVon EverandGuidelines for Enabling Conditions and Conditional Modifiers in Layer of Protection AnalysisNoch keine Bewertungen
- An Applied Guide to Water and Effluent Treatment Plant DesignVon EverandAn Applied Guide to Water and Effluent Treatment Plant DesignBewertung: 5 von 5 Sternen5/5 (4)
- Robotics: Designing the Mechanisms for Automated MachineryVon EverandRobotics: Designing the Mechanisms for Automated MachineryBewertung: 4.5 von 5 Sternen4.5/5 (8)
- Guidelines for Developing Quantitative Safety Risk CriteriaVon EverandGuidelines for Developing Quantitative Safety Risk CriteriaNoch keine Bewertungen
- Chemical Process Safety: Learning from Case HistoriesVon EverandChemical Process Safety: Learning from Case HistoriesBewertung: 4 von 5 Sternen4/5 (14)
- Guidelines for Engineering Design for Process SafetyVon EverandGuidelines for Engineering Design for Process SafetyNoch keine Bewertungen
- Perfume Engineering: Design, Performance and ClassificationVon EverandPerfume Engineering: Design, Performance and ClassificationBewertung: 4 von 5 Sternen4/5 (5)
- Temperature-Responsive Polymers: Chemistry, Properties, and ApplicationsVon EverandTemperature-Responsive Polymers: Chemistry, Properties, and ApplicationsNoch keine Bewertungen
- The HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesVon EverandThe HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesNoch keine Bewertungen
- Bow Ties in Risk Management: A Concept Book for Process SafetyVon EverandBow Ties in Risk Management: A Concept Book for Process SafetyNoch keine Bewertungen