Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Simple Linear RegressionDokument55 SeitenSimple Linear RegressionPatrick HernandezNoch keine Bewertungen
- COT 2 Reading and Writing Q4Dokument4 SeitenCOT 2 Reading and Writing Q4Romy Sales Grande Jr.Noch keine Bewertungen
- The Ethics of Consumer Protection & Marketing: Ecture YnopsisDokument6 SeitenThe Ethics of Consumer Protection & Marketing: Ecture Ynopsiskuashask2Noch keine Bewertungen
- Lesson 2.5 Reading Strategies - Narrative TextsDokument34 SeitenLesson 2.5 Reading Strategies - Narrative Textsjannica yzabelNoch keine Bewertungen
- Railway Fatalities in South West MumbaiDokument12 SeitenRailway Fatalities in South West MumbaiAwpan SabaleNoch keine Bewertungen
- Lesson Plan in Oral Communication in ContextDokument2 SeitenLesson Plan in Oral Communication in ContextYoutube TutorialsNoch keine Bewertungen
- Introduction To Marketing ManagementDokument24 SeitenIntroduction To Marketing ManagementDrRuchi GargNoch keine Bewertungen
- 7.2.5 APQP Phase 2 Checklist Dec 2013Dokument21 Seiten7.2.5 APQP Phase 2 Checklist Dec 2013Mani Rathinam RajamaniNoch keine Bewertungen
- Optimal Voltage RegulatorDokument8 SeitenOptimal Voltage RegulatorARVINDNoch keine Bewertungen
- Sample of Interview Protocol - Questions Adopted From Timmons 1994Dokument2 SeitenSample of Interview Protocol - Questions Adopted From Timmons 1994Ash RafNoch keine Bewertungen
- SM-A315G - LA Electrical Part List Galaxy A31Dokument10 SeitenSM-A315G - LA Electrical Part List Galaxy A31liquidNoch keine Bewertungen
- The Art of Fishing PDFDokument27 SeitenThe Art of Fishing PDFsilentkillersbh1729Noch keine Bewertungen
- Rim and Face - Alignment KnowledgeDokument19 SeitenRim and Face - Alignment Knowledgevj kumarNoch keine Bewertungen
- SUBIECTE - LICEU EnglezaDokument34 SeitenSUBIECTE - LICEU EnglezaElla Petrescu VasiiNoch keine Bewertungen
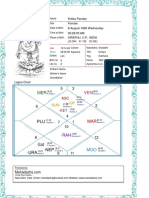
- Kritika Pandey (Kaushambi)Dokument15 SeitenKritika Pandey (Kaushambi)nishink9Noch keine Bewertungen
- Lecture Slides: Elementary StatisticsDokument129 SeitenLecture Slides: Elementary StatisticsHassan HusseinNoch keine Bewertungen
- Planning For Big Data PDFDokument88 SeitenPlanning For Big Data PDFexelius100% (1)
- 05 AccelerationDownIncline-2Dokument4 Seiten05 AccelerationDownIncline-2PeterNoch keine Bewertungen
- Chapter 3 - Basic Statistical ConceptsDokument16 SeitenChapter 3 - Basic Statistical ConceptsChristian Alfred VillenaNoch keine Bewertungen
- Practical Research 1 Qualitative 2Dokument112 SeitenPractical Research 1 Qualitative 2ZleCerboAtienza100% (3)
- Software Requirements Specification TemplateDokument6 SeitenSoftware Requirements Specification TemplatekkrrrsssNoch keine Bewertungen
- The Role of Lay People in The Production and Dissemination of Scientific KnowledgeDokument15 SeitenThe Role of Lay People in The Production and Dissemination of Scientific KnowledgeanferrufoNoch keine Bewertungen
- Polite Form and Verb Stems: Not Being Rude in JapanDokument84 SeitenPolite Form and Verb Stems: Not Being Rude in Japaneulea larkaroNoch keine Bewertungen
- MaseeiDokument34 SeitenMaseeivikrant100% (1)
- Quantification of Organic Acids by HPLCDokument5 SeitenQuantification of Organic Acids by HPLCLee HaronNoch keine Bewertungen
- VoIPmonitor Sniffer Manual v5Dokument19 SeitenVoIPmonitor Sniffer Manual v5Allan PadillaNoch keine Bewertungen
- Ventures Priamry Heritage-Social StudiesDokument128 SeitenVentures Priamry Heritage-Social StudiesWryter Business100% (2)
- POL 203 Intro To Western Political PhilosophyDokument202 SeitenPOL 203 Intro To Western Political PhilosophyShan Ali Shah100% (1)
- Documentation 040Dokument148 SeitenDocumentation 040proxemicNoch keine Bewertungen
- Genpact Leansixsigma Training OfferingDokument4 SeitenGenpact Leansixsigma Training OfferingSwamy NunnaNoch keine Bewertungen