Das könnte Ihnen auch gefallen
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementVon EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNoch keine Bewertungen
- Summary of Andrew J. Wakefield's Waging War On The Autistic ChildVon EverandSummary of Andrew J. Wakefield's Waging War On The Autistic ChildNoch keine Bewertungen
- Update On Diarrhea - Peds in Rev 2016Dokument12 SeitenUpdate On Diarrhea - Peds in Rev 2016TriLightNoch keine Bewertungen
- Update On DiarrheaDokument12 SeitenUpdate On DiarrheantnquynhproNoch keine Bewertungen
- 6DehydrationRefArticle6 PDFDokument11 Seiten6DehydrationRefArticle6 PDFMaya LarasNoch keine Bewertungen
- Gastroenteritis: AcuteDokument11 SeitenGastroenteritis: AcuteKhuswatun HasanahNoch keine Bewertungen
- Acute Diarrhea in Adults and ChildrenDokument30 SeitenAcute Diarrhea in Adults and ChildrenM Isyhaduul IslamNoch keine Bewertungen
- Acute Gastroenteritis in ChildrenDokument24 SeitenAcute Gastroenteritis in ChildrenramwshNoch keine Bewertungen
- GASTROENTERITISDokument24 SeitenGASTROENTERITISKevin VillaranteNoch keine Bewertungen
- Diarréia em Potros - 2007Dokument3 SeitenDiarréia em Potros - 2007thiago.veterinariaNoch keine Bewertungen
- Guia EDA EuropeaDokument6 SeitenGuia EDA EuropeaCarlos HurtadoNoch keine Bewertungen
- Approach To The Child With Acute Diarrhea in Resource-Limited Countries - UpToDateDokument17 SeitenApproach To The Child With Acute Diarrhea in Resource-Limited Countries - UpToDateNedelcu MirunaNoch keine Bewertungen
- The Vomiting Child PDFDokument4 SeitenThe Vomiting Child PDFJos ArnoNoch keine Bewertungen
- Gastro PDFDokument6 SeitenGastro PDFAvrianne NicoleNoch keine Bewertungen
- Wa0018.Dokument7 SeitenWa0018.mahesh shindeNoch keine Bewertungen
- Pro BioticDokument6 SeitenPro BioticYoga Zunandy PratamaNoch keine Bewertungen
- Ojepi 2021062511285512Dokument15 SeitenOjepi 2021062511285512galuhskripsianberhasilNoch keine Bewertungen
- (Nelsons 21st) Acute GastroenteritisDokument21 Seiten(Nelsons 21st) Acute GastroenteritisLara Patricia TamsiNoch keine Bewertungen
- Pro BioticDokument6 SeitenPro BioticRizki WahyuniNoch keine Bewertungen
- CPG AID - Pocket Guide.v7 PDFDokument31 SeitenCPG AID - Pocket Guide.v7 PDFR ParkNoch keine Bewertungen
- Ochoa 2004Dokument8 SeitenOchoa 2004Syarifah Maryam AlydrusNoch keine Bewertungen
- Calamba Rle112 Reading-2Dokument2 SeitenCalamba Rle112 Reading-2CHRISTIAN CALAMBANoch keine Bewertungen
- GastroenteritisDokument2 SeitenGastroenteritisabhieghailNoch keine Bewertungen
- Acute Infectious Diarrhea and Gastroenteritis in ChildrenDokument12 SeitenAcute Infectious Diarrhea and Gastroenteritis in ChildrenLuis AlfredoNoch keine Bewertungen
- Acute Diarrhea: Evidence-Based Management: Review ArticleDokument8 SeitenAcute Diarrhea: Evidence-Based Management: Review ArticlevanialinNoch keine Bewertungen
- Diarrea Cronica PDFDokument7 SeitenDiarrea Cronica PDFArturo Castro UrbinaNoch keine Bewertungen
- Case (Acute Gastroenteritis) Group 4Dokument36 SeitenCase (Acute Gastroenteritis) Group 4EljhayrosNoch keine Bewertungen
- Nutritional Management of Acute Diarrhea: Global Issues in Pediatric NutritionDokument5 SeitenNutritional Management of Acute Diarrhea: Global Issues in Pediatric NutritionKristina Joy HerlambangNoch keine Bewertungen
- Effect of Probiotic Treatment On Acute Diarrhea in Childhood ARTICLE INFODokument6 SeitenEffect of Probiotic Treatment On Acute Diarrhea in Childhood ARTICLE INFOKhalila IzdiharNoch keine Bewertungen
- Pediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapDokument10 SeitenPediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapvgmanjunathNoch keine Bewertungen
- Chronic DiarrheaDokument17 SeitenChronic Diarrheafatimah zahraaNoch keine Bewertungen
- Klasifikasi Diare Pada AnakDokument15 SeitenKlasifikasi Diare Pada AnakTia UtamiNoch keine Bewertungen
- Campylobacter Jejuni, Salmonella, Clostridium Diffi CileDokument14 SeitenCampylobacter Jejuni, Salmonella, Clostridium Diffi CileMary Glydeane CanimoNoch keine Bewertungen
- AGE ReadingsDokument6 SeitenAGE ReadingseljhayrosNoch keine Bewertungen
- Infant Gastroesophageal Reflux Disease Management Consensus 2024Dokument8 SeitenInfant Gastroesophageal Reflux Disease Management Consensus 2024Dayana FajardoNoch keine Bewertungen
- Risk Factors of Persistent Diarrhea in Children BeDokument5 SeitenRisk Factors of Persistent Diarrhea in Children Beahtianti ramdani sahputriNoch keine Bewertungen
- Management of Acute DiarrheaDokument38 SeitenManagement of Acute DiarrheaHooria. BariNoch keine Bewertungen
- The Role of Probiotics in Prevention PDFDokument9 SeitenThe Role of Probiotics in Prevention PDFFernandoNoch keine Bewertungen
- Global Diarrhea 508 CDokument18 SeitenGlobal Diarrhea 508 CNajib ZulkifliNoch keine Bewertungen
- Overview of The Causes of Chronic Diarrhea in Children in Resource-Rich Settings - Uptodate FreeDokument19 SeitenOverview of The Causes of Chronic Diarrhea in Children in Resource-Rich Settings - Uptodate Freekhaled khaterNoch keine Bewertungen
- Case2 AnswerDokument5 SeitenCase2 AnswerKATHERINE CANCIONoch keine Bewertungen
- Acute Infectious Diarrhea in Children: Continuing Medical EducationDokument11 SeitenAcute Infectious Diarrhea in Children: Continuing Medical EducationkhorikNoch keine Bewertungen
- Bacterial Diarrhea: Clinical PracticeDokument10 SeitenBacterial Diarrhea: Clinical PracticeReno WaisyahNoch keine Bewertungen
- Diarrhea EDokument1 SeiteDiarrhea Eabdalballah1151Noch keine Bewertungen
- In Ammatory Bowel Disease: Educational GapsDokument14 SeitenIn Ammatory Bowel Disease: Educational GapsMonica LeeNoch keine Bewertungen
- Parrish July 2013Dokument7 SeitenParrish July 2013Tada MinionNoch keine Bewertungen
- H PyloriDokument10 SeitenH Pylorividia_psNoch keine Bewertungen
- Shigella 261 FullDokument4 SeitenShigella 261 FullDditelmNoch keine Bewertungen
- Persistent DiarrheaDokument7 SeitenPersistent DiarrheaDickyNoch keine Bewertungen
- Curbing Diarrhea in ChildrenDokument8 SeitenCurbing Diarrhea in ChildrenKIU PUBLICATION AND EXTENSIONNoch keine Bewertungen
- Bacterial Diarrhea: Clinical PracticeDokument10 SeitenBacterial Diarrhea: Clinical PracticeHugo MarizNoch keine Bewertungen
- Age: Acute Gastroenteritis: Kamar H. Callanga // Jashmir Joyce F. BanuaDokument15 SeitenAge: Acute Gastroenteritis: Kamar H. Callanga // Jashmir Joyce F. BanuaKamar CallangaNoch keine Bewertungen
- Guarino 2014Dokument21 SeitenGuarino 2014ChangNoch keine Bewertungen
- Presentation 3Dokument14 SeitenPresentation 3olayemi morakinyoNoch keine Bewertungen
- Acute Diare DiaseseDokument9 SeitenAcute Diare DiaseseAnonymous l3X3jf0NPNoch keine Bewertungen
- Diarrhea ATPDokument42 SeitenDiarrhea ATPsoni syangboNoch keine Bewertungen
- Constipation ArticleDokument6 SeitenConstipation ArticleDivyang BhaiNoch keine Bewertungen
- Advances in Evaluation of Chronic Diarrhea in InfantDokument21 SeitenAdvances in Evaluation of Chronic Diarrhea in InfantDr. Faten AlKatebNoch keine Bewertungen
- Acute Viral Gastroenteritis in Children in Resource-Abundant Countries - Management and Prevention - UpToDateDokument31 SeitenAcute Viral Gastroenteritis in Children in Resource-Abundant Countries - Management and Prevention - UpToDatealejandrohdezh007Noch keine Bewertungen
- Enf Diarreica AdultosDokument9 SeitenEnf Diarreica AdultosaesquiviaplazaNoch keine Bewertungen
- Epoc Gold 2017Dokument32 SeitenEpoc Gold 2017sanlupinNoch keine Bewertungen
- In The Clinic ITUDokument16 SeitenIn The Clinic ITUsanlupinNoch keine Bewertungen
- (Piano Sheet) Sonata Arctica - TallulahDokument7 Seiten(Piano Sheet) Sonata Arctica - TallulahAlee__50% (2)
- (Piano Sheet) Sonata Arctica - TallulahDokument7 Seiten(Piano Sheet) Sonata Arctica - TallulahAlee__50% (2)
- (Piano Sheet) Sonata Arctica - TallulahDokument7 Seiten(Piano Sheet) Sonata Arctica - TallulahAlee__50% (2)
- Chop SueyDokument7 SeitenChop Sueyjohn17727100% (1)
- Faith No More - Easy Like Sunday MorningDokument3 SeitenFaith No More - Easy Like Sunday Morningcarlosmoreiracarlos75% (4)
- Trees in IndiaDokument43 SeitenTrees in IndiaAr Archana PrabakaranNoch keine Bewertungen
- LorazepamDokument4 SeitenLorazepamapi-3797941Noch keine Bewertungen
- Source: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical EthicsDokument67 SeitenSource: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical Ethicsjamestery0% (1)
- Turpentine Oil Poisoning MedlinePlus Medical EncyclopediaDokument4 SeitenTurpentine Oil Poisoning MedlinePlus Medical Encyclopediapiemar10Noch keine Bewertungen
- Battle Mind An OverviewDokument7 SeitenBattle Mind An OverviewUzair UmairNoch keine Bewertungen
- Pga CetDokument31 SeitenPga CetDrHassan Ahmed ShaikhNoch keine Bewertungen
- Bucks County Courier Times 01-03-2010Dokument90 SeitenBucks County Courier Times 01-03-2010ssinger04Noch keine Bewertungen
- Varma Varmam Marma Book Full Color in English - VKRC Vol 2 Book S Ramesh Babu - Free PDF DownloadDokument14 SeitenVarma Varmam Marma Book Full Color in English - VKRC Vol 2 Book S Ramesh Babu - Free PDF DownloadS Ramesh BabuNoch keine Bewertungen
- Abdominal BandagingDokument34 SeitenAbdominal BandagingStephanie Cyrelle Jane BacaniNoch keine Bewertungen
- Ground Floor Plan Sheet 2Dokument1 SeiteGround Floor Plan Sheet 2riteshNoch keine Bewertungen
- CAPNOGRAPHYDokument10 SeitenCAPNOGRAPHYJessica GuzmanNoch keine Bewertungen
- Hospitals in KochiDokument6 SeitenHospitals in Kochianandrv86Noch keine Bewertungen
- AP Research PresentationDokument26 SeitenAP Research PresentationCameron SherryNoch keine Bewertungen
- Mike's Recommended Books For Paramedic StudentsDokument3 SeitenMike's Recommended Books For Paramedic StudentsMichael WilsonNoch keine Bewertungen
- Poster Role of Clinical Exome SequencingDokument1 SeitePoster Role of Clinical Exome SequencingLudy ArfanNoch keine Bewertungen
- Sistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022Dokument13 SeitenSistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022vera kusunyadewiNoch keine Bewertungen
- VibhorDokument21 SeitenVibhorNeha ShuklaNoch keine Bewertungen
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDokument2 SeitenProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNoch keine Bewertungen
- Windy WigaDokument2 SeitenWindy WigaWindy wigaNoch keine Bewertungen
- Daftar Pustaka NewDokument2 SeitenDaftar Pustaka NewRini LianingsihNoch keine Bewertungen
- +bashkir State Medical UniversityDokument2 Seiten+bashkir State Medical UniversityCB SharmaNoch keine Bewertungen
- Health Sector EHSMS Requirements-June 2012Dokument31 SeitenHealth Sector EHSMS Requirements-June 2012Aya MahmoudNoch keine Bewertungen
- 1005 Hemorrhage ControlDokument88 Seiten1005 Hemorrhage ControlZainescu Dan100% (2)
- Binge EatingDokument18 SeitenBinge EatingIuliana IgnatNoch keine Bewertungen
- 2023 Welcome Event SOPDokument13 Seiten2023 Welcome Event SOPNur Adila Binti AzmanNoch keine Bewertungen
- PLI Proposal FormDokument8 SeitenPLI Proposal FormPalakala NagarjunaNoch keine Bewertungen
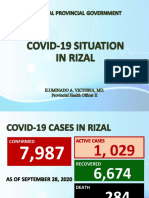
- Covid19 Situation in RizalDokument23 SeitenCovid19 Situation in RizalToni Quitalig GamezNoch keine Bewertungen
- Be Happy Healthy Wealthy SAMPLEDokument30 SeitenBe Happy Healthy Wealthy SAMPLERosie GonzalesNoch keine Bewertungen
- HFS PHILIPPINES, INC., G.R. No. 168716 Ruben T. Del Rosario and Ium Shipmanagement As, Petitioners, Ronaldo R. Pilar, Respondent. PromulgatedDokument8 SeitenHFS PHILIPPINES, INC., G.R. No. 168716 Ruben T. Del Rosario and Ium Shipmanagement As, Petitioners, Ronaldo R. Pilar, Respondent. PromulgateddanexrainierNoch keine Bewertungen
- Products Ayurvedic Medicines Cosmetics Herbs Medicinal Plants Cultivation Processing Herbal Extract Natural Plant Extracts Ayurvedic Pharma Ayurvedic Products Herbal Medicine Herbal Cosmetics Ayurvedic FormulDokument2 SeitenProducts Ayurvedic Medicines Cosmetics Herbs Medicinal Plants Cultivation Processing Herbal Extract Natural Plant Extracts Ayurvedic Pharma Ayurvedic Products Herbal Medicine Herbal Cosmetics Ayurvedic FormulAnonymous bvQJjRNoch keine Bewertungen