Das könnte Ihnen auch gefallen
- Psychotropic Drugs, Drug Abuse Drug Dependence - FinalDokument26 SeitenPsychotropic Drugs, Drug Abuse Drug Dependence - Finalmulengamordecai92Noch keine Bewertungen
- Drug Addiction & The BrainDokument45 SeitenDrug Addiction & The BrainGaurav JainNoch keine Bewertungen
- Drug Abuse, Dependence, AddictionDokument36 SeitenDrug Abuse, Dependence, AddictionIan100% (1)
- AntidepressantsDokument59 SeitenAntidepressantsanon_189054600100% (2)
- Second Gen AtipsychoticDokument34 SeitenSecond Gen Atipsychoticemamma hashirNoch keine Bewertungen
- NaltrexoneDokument44 SeitenNaltrexonePrag GK SubediNoch keine Bewertungen
- Neurobiology of AddictionDokument48 SeitenNeurobiology of Addictionisland.sidle0nNoch keine Bewertungen
- Anti Epileptic AgentsDokument64 SeitenAnti Epileptic AgentsPrincess VanquirayNoch keine Bewertungen
- An Tide Prees AntDokument38 SeitenAn Tide Prees Antnamah odatNoch keine Bewertungen
- Psychotropic DrugsDokument81 SeitenPsychotropic DrugsJoan100% (2)
- PAws Samsha PDFDokument8 SeitenPAws Samsha PDFAnonymous JS9PXY2100% (1)
- Substance Related DisordersDokument18 SeitenSubstance Related DisordersBEA RADANoch keine Bewertungen
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDokument16 SeitenName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNoch keine Bewertungen
- Central Nervous System StimulantsDokument20 SeitenCentral Nervous System StimulantsAn LoNoch keine Bewertungen
- Neurophysiology of AddictionDokument11 SeitenNeurophysiology of AddictionShivan A.C.Noch keine Bewertungen
- The Key To Freeing Your Life From AddictionDokument22 SeitenThe Key To Freeing Your Life From AddictionBrainyBlondieNoch keine Bewertungen
- Addiction: by Wan Mohd Fikri Bin Wan Mohd NasirDokument26 SeitenAddiction: by Wan Mohd Fikri Bin Wan Mohd NasirMimi FatinNoch keine Bewertungen
- HES-005-Session-9-SASDokument9 SeitenHES-005-Session-9-SASDave Ortiz Robert MaglasangNoch keine Bewertungen
- Principles of Drug Abuse Spring 2021Dokument33 SeitenPrinciples of Drug Abuse Spring 2021Fatma HishamNoch keine Bewertungen
- Other Addictive Substances - SBADokument10 SeitenOther Addictive Substances - SBADivijaa More100% (1)
- Recent Advances in Understanding and Management of Benzodiazepine, Cannabinoids & Tobacco DependenceDokument54 SeitenRecent Advances in Understanding and Management of Benzodiazepine, Cannabinoids & Tobacco Dependencestpeter_agraNoch keine Bewertungen
- Sedative-Hypnotic Drugs: Department of Pharmacology Zhang YanmeiDokument30 SeitenSedative-Hypnotic Drugs: Department of Pharmacology Zhang YanmeiKAVITA HOODANoch keine Bewertungen
- 3 - Lec - PahrmaDokument45 Seiten3 - Lec - PahrmaDr Nimra MurtazaNoch keine Bewertungen
- The Neuroscience of Addiction: Understanding the Brain's Reward SystemVon EverandThe Neuroscience of Addiction: Understanding the Brain's Reward SystemNoch keine Bewertungen
- Sedative-Hypnotic DrugsDokument30 SeitenSedative-Hypnotic DrugsdrfatimarizNoch keine Bewertungen
- Lecture 2 (Psychotropic Drugs)Dokument17 SeitenLecture 2 (Psychotropic Drugs)ahmadslayman1Noch keine Bewertungen
- SU Lec 7 Pharma 2 PDFDokument24 SeitenSU Lec 7 Pharma 2 PDFGamal EdrisNoch keine Bewertungen
- Anti Epileptic AgentsDokument78 SeitenAnti Epileptic AgentsPrincess VanquirayNoch keine Bewertungen
- Drug Addiction: Physical Dependence Is A State of Adaptation of The Organism To The Presence of The Drug and IsDokument9 SeitenDrug Addiction: Physical Dependence Is A State of Adaptation of The Organism To The Presence of The Drug and IsMehar KhanNoch keine Bewertungen
- How Do People Intentionally Alter Their States of Consciousness?Dokument9 SeitenHow Do People Intentionally Alter Their States of Consciousness?Filullah Fil AlamNoch keine Bewertungen
- Substance RelatedDokument12 SeitenSubstance RelatedJoyce VillalesNoch keine Bewertungen
- Antiepileptic Drugs (Anti-Seizure Drugs) - IDokument39 SeitenAntiepileptic Drugs (Anti-Seizure Drugs) - Inouramansour235Noch keine Bewertungen
- Depression Disease: Represented byDokument36 SeitenDepression Disease: Represented byanisahanifatinrNoch keine Bewertungen
- Understanding The Disease of AddictionDokument7 SeitenUnderstanding The Disease of AddictionJoão MaiaNoch keine Bewertungen
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanDokument51 SeitenPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganNoch keine Bewertungen
- 3tobacco Addiction 2002Dokument29 Seiten3tobacco Addiction 2002Antonio BernardNoch keine Bewertungen
- Pharmacology of AntidepressantsDokument28 SeitenPharmacology of Antidepressantsحيدر كريم سعيد حمزهNoch keine Bewertungen
- Treatment of Common Mental DisordersDokument77 SeitenTreatment of Common Mental DisordersnelsonNoch keine Bewertungen
- Antidepressants (Igor Iezhitsa) Students Copy (ME219)Dokument40 SeitenAntidepressants (Igor Iezhitsa) Students Copy (ME219)Zobayer AhmedNoch keine Bewertungen
- AntidepressantsDokument14 SeitenAntidepressantsTuwaij SarrarNoch keine Bewertungen
- WEEK 6 7-CNS Medications StudentDokument83 SeitenWEEK 6 7-CNS Medications Studentx8jdbj5gphNoch keine Bewertungen
- Psychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditDokument99 SeitenPsychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditCITRA AYU APRILIANoch keine Bewertungen
- Somatic TherapiesDokument170 SeitenSomatic TherapiesDelyn Gamutan Millan100% (2)
- Week 11 Part 2Dokument37 SeitenWeek 11 Part 2Aafreen AhmedNoch keine Bewertungen
- Module 8Dokument5 SeitenModule 8Yuki Xairah TunayNoch keine Bewertungen
- The Affective DisordersDokument22 SeitenThe Affective DisordersMUHD SUHAILNoch keine Bewertungen
- Ab Psych 2 FinalsDokument13 SeitenAb Psych 2 FinalsGabrielle Anne AbadNoch keine Bewertungen
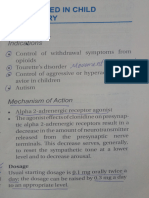
- Drugs Used in Child Psychiatry (MHN)Dokument2 SeitenDrugs Used in Child Psychiatry (MHN)fathima7910Noch keine Bewertungen
- Tutorial 4.4Dokument4 SeitenTutorial 4.4Rosa FinizioNoch keine Bewertungen
- AntidepressantsDokument4 SeitenAntidepressantsSalman HabeebNoch keine Bewertungen
- Pharmacology 2Dokument37 SeitenPharmacology 2jekeri bekeriNoch keine Bewertungen
- Sedative Hypnotic DETOX For PHYSICIANS 2-11-14Dokument19 SeitenSedative Hypnotic DETOX For PHYSICIANS 2-11-14Frank Raymond100% (1)
- Antidepressant AgentsDokument66 SeitenAntidepressant AgentsKryzza LeizellNoch keine Bewertungen
- 7 - Drugs Used in ParkinsonDokument47 Seiten7 - Drugs Used in ParkinsonSara AbbasNoch keine Bewertungen
- Antidepressant DrugsDokument15 SeitenAntidepressant DrugsDr. Mushfique Imtiaz ChowdhuryNoch keine Bewertungen
- Cns Pharmacology For Pc-IIDokument135 SeitenCns Pharmacology For Pc-IItinsaeworkineh976Noch keine Bewertungen
- Nervous System PART 2Dokument69 SeitenNervous System PART 2Jeyan BoncavilNoch keine Bewertungen
- Antidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyDokument38 SeitenAntidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyVinod GuruNoch keine Bewertungen
- Matrix - Roadmap To RecoveryDokument3 SeitenMatrix - Roadmap To RecoveryCCNoch keine Bewertungen
- Summary of John D. Preston, John H. O'Neal, Mary C. Talaga & Bret A. Moore's Handbook of Clinical Psychopharmacology for TherapistsVon EverandSummary of John D. Preston, John H. O'Neal, Mary C. Talaga & Bret A. Moore's Handbook of Clinical Psychopharmacology for TherapistsNoch keine Bewertungen
- Psyc1022 Topic 5Dokument6 SeitenPsyc1022 Topic 5PatriciaNoch keine Bewertungen
- Psyc1022 Topic 6Dokument12 SeitenPsyc1022 Topic 6PatriciaNoch keine Bewertungen
- Psyc1022 Topic 8Dokument4 SeitenPsyc1022 Topic 8PatriciaNoch keine Bewertungen
- Psyc1022 Topic 4Dokument4 SeitenPsyc1022 Topic 4PatriciaNoch keine Bewertungen
- Psyc1022 Topic 3Dokument5 SeitenPsyc1022 Topic 3PatriciaNoch keine Bewertungen
- Psyc1022 Topic 2Dokument2 SeitenPsyc1022 Topic 2PatriciaNoch keine Bewertungen
- Psyc1022 Topic 1Dokument8 SeitenPsyc1022 Topic 1PatriciaNoch keine Bewertungen
- MATH1151 Course OutlineDokument29 SeitenMATH1151 Course OutlinePatriciaNoch keine Bewertungen
- ACCT1511 Accounting and Financial Management 1B S22016Dokument20 SeitenACCT1511 Accounting and Financial Management 1B S22016PatriciaNoch keine Bewertungen
- ACCT1501 Course OutlineDokument23 SeitenACCT1501 Course OutlinePatriciaNoch keine Bewertungen
- Week 8 Monday 12-1 ClassDokument2 SeitenWeek 8 Monday 12-1 ClassPatriciaNoch keine Bewertungen
- Algebra 1 Expansion of BracketsDokument1 SeiteAlgebra 1 Expansion of BracketsPatriciaNoch keine Bewertungen
- ECON1102 Macroeconomics 1 Part A S12016Dokument12 SeitenECON1102 Macroeconomics 1 Part A S12016PatriciaNoch keine Bewertungen
- ACTL1101 CourseOutlineA S2 2016Dokument14 SeitenACTL1101 CourseOutlineA S2 2016PatriciaNoch keine Bewertungen
- Substance Abuse: Alcohol Abuse Case DescriptionDokument28 SeitenSubstance Abuse: Alcohol Abuse Case DescriptionMaria Fatima MagsinoNoch keine Bewertungen
- Cognitive-Behavioral Treatment of Depression: A Three-Stage Model To Guide Treatment PlanningDokument9 SeitenCognitive-Behavioral Treatment of Depression: A Three-Stage Model To Guide Treatment PlanningRija ChoudhryNoch keine Bewertungen
- Treatment of Tobacco Use and Dependence: The Role of The Dental ProfessionalDokument17 SeitenTreatment of Tobacco Use and Dependence: The Role of The Dental ProfessionalAinur 'iin' RahmahNoch keine Bewertungen
- Addiction Research & Therapy: Psychological Management of CravingDokument3 SeitenAddiction Research & Therapy: Psychological Management of CravingNorma FloresNoch keine Bewertungen
- A Case On Typhoid Fever: Group 4Dokument27 SeitenA Case On Typhoid Fever: Group 4Donzzkie DonNoch keine Bewertungen
- Challenging The Brain Disease Model of Addiction European Launch of The Addiction Theory NetworkDokument8 SeitenChallenging The Brain Disease Model of Addiction European Launch of The Addiction Theory NetworkJonatan Daniel Díaz MárquezNoch keine Bewertungen
- CBT KaddenDokument28 SeitenCBT KaddenAbhik SahaNoch keine Bewertungen
- Psychosocialintervention 2Dokument172 SeitenPsychosocialintervention 2Roh Jiten100% (1)
- Neurobiology of Addiction: Toward The Development of New TherapiesDokument16 SeitenNeurobiology of Addiction: Toward The Development of New Therapiesguessimfloatin GNoch keine Bewertungen
- Asam Criteria PDFDokument14 SeitenAsam Criteria PDFFelipe Rangel Hassey83% (6)
- Drug Addict Case ReportDokument18 SeitenDrug Addict Case ReportHajra KhanNoch keine Bewertungen
- Am J Clin Nutr-1990-Kayman-800-7 PDFDokument8 SeitenAm J Clin Nutr-1990-Kayman-800-7 PDFGindi Cinintia AsmarantakaNoch keine Bewertungen
- Person Centered Planning vs. Provider Centered PlanningDokument5 SeitenPerson Centered Planning vs. Provider Centered PlanningRobert JohnsonNoch keine Bewertungen
- SUD 3: Alcohol Use Disorder TreatmentDokument12 SeitenSUD 3: Alcohol Use Disorder TreatmentMike NakhlaNoch keine Bewertungen
- Predictor Factor On Relapse Among Former AddictsDokument12 SeitenPredictor Factor On Relapse Among Former AddictsDevika OktavianiNoch keine Bewertungen
- Research Paper Grade10Dokument24 SeitenResearch Paper Grade10shayeNoch keine Bewertungen
- Addiction Recovery Through Photovoice Qualitative StudyDokument18 SeitenAddiction Recovery Through Photovoice Qualitative Studylapkas donjuanNoch keine Bewertungen
- Addiction Homework AssignmentsDokument4 SeitenAddiction Homework Assignmentsvnwmruilf100% (1)
- ASAM 101: How To Complete The ASAM Placement FormDokument24 SeitenASAM 101: How To Complete The ASAM Placement FormMistor Dupois Williams100% (2)
- Stress and Gastritis Relationship at Public Health ServiceDokument6 SeitenStress and Gastritis Relationship at Public Health Serviceoliffasalma atthahirohNoch keine Bewertungen
- Exercise Addiction A Literature ReviewDokument7 SeitenExercise Addiction A Literature Reviewc5sq1b48100% (1)
- SBWCC Offender HandbookDokument20 SeitenSBWCC Offender HandbookMark ReinhardtNoch keine Bewertungen
- Recovery High Schools: A Descriptive Study of School Programs and StudentsDokument30 SeitenRecovery High Schools: A Descriptive Study of School Programs and StudentsThe Stacie Mathewson FoundationNoch keine Bewertungen
- Aisha Isyaku Term PaperDokument27 SeitenAisha Isyaku Term PaperUsman Ahmad TijjaniNoch keine Bewertungen
- A Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalDokument66 SeitenA Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalUsman Ahmad Tijjani100% (2)
- Physiology & Behavior: Mark E. BoutonDokument8 SeitenPhysiology & Behavior: Mark E. BoutonjsaccuzzoNoch keine Bewertungen
- Relapse Processes After The Extinction of Instrumental Learning: Renewal, Resurgence, and ReacquisitionDokument12 SeitenRelapse Processes After The Extinction of Instrumental Learning: Renewal, Resurgence, and ReacquisitionjsaccuzzoNoch keine Bewertungen
- Efektifitas Pemberian Family Psychoeducation (Fpe) Terhadap Kepatuhan Minum Obat Penderita Skizofrenia Di Kota KediriDokument5 SeitenEfektifitas Pemberian Family Psychoeducation (Fpe) Terhadap Kepatuhan Minum Obat Penderita Skizofrenia Di Kota KediriTuan AriefNoch keine Bewertungen
- DocumentDokument10 SeitenDocumentCr Zaidi Abu HassanNoch keine Bewertungen
- TC Primer PDFDokument19 SeitenTC Primer PDFJais CampanillaNoch keine Bewertungen