Das könnte Ihnen auch gefallen
- Article: Effects of A Mediterranean-Style Diet On Cardiovascular Risk FactorsDokument15 SeitenArticle: Effects of A Mediterranean-Style Diet On Cardiovascular Risk FactorsBunga dewanggi NugrohoNoch keine Bewertungen
- J of Clinical Hypertension - 2021 - Verma - Non Pharmacological Management of HypertensionDokument9 SeitenJ of Clinical Hypertension - 2021 - Verma - Non Pharmacological Management of HypertensionIsrael LovechildNoch keine Bewertungen
- Review Article: Functional Foods and Nutraceuticals in The Primary Prevention of Cardiovascular DiseasesDokument17 SeitenReview Article: Functional Foods and Nutraceuticals in The Primary Prevention of Cardiovascular DiseasesUmar AliNoch keine Bewertungen
- Mediterranean Diet, Vitamin D, and Hypercaloric, HyperproteicDokument16 SeitenMediterranean Diet, Vitamin D, and Hypercaloric, HyperproteicFransiska FranshuidNoch keine Bewertungen
- Non Pharmacological Management of Hypertension - PMCDokument16 SeitenNon Pharmacological Management of Hypertension - PMCBrian TaylorNoch keine Bewertungen
- Effect of Alhagi Maurorum or Gloularia Alypum On Lipid Profile of Experimentally Induced Hypercholesteremic Rats and On Blood Pressure of Experimentally Induced Hypertensive RatsDokument8 SeitenEffect of Alhagi Maurorum or Gloularia Alypum On Lipid Profile of Experimentally Induced Hypercholesteremic Rats and On Blood Pressure of Experimentally Induced Hypertensive RatsMediterr J Pharm Pharm SciNoch keine Bewertungen
- 2016 Lacroix S Nutrition in CV RehabDokument7 Seiten2016 Lacroix S Nutrition in CV RehabHumamuddinNoch keine Bewertungen
- Course NB 2 Nutrition in CVDDokument26 SeitenCourse NB 2 Nutrition in CVDАнна ДабежаNoch keine Bewertungen
- Fitoetal 2016 Nutrients Review FINALDokument13 SeitenFitoetal 2016 Nutrients Review FINALAndrés Felipe Zapata MurielNoch keine Bewertungen
- Articulo Dislipidemias 2Dokument18 SeitenArticulo Dislipidemias 2DANIELA CALDERON SAGAHONNoch keine Bewertungen
- Tovar Et Al-2017-Molecular Nutrition & Food ResearchDokument12 SeitenTovar Et Al-2017-Molecular Nutrition & Food ResearchRal T. BerensNoch keine Bewertungen
- A Narrative Review of Dietary Approaches Fo Kidney Transplant PatientsDokument11 SeitenA Narrative Review of Dietary Approaches Fo Kidney Transplant PatientsGabriel Abreu PattoNoch keine Bewertungen
- 1 s2.0 S0022316622164783 MainDokument10 Seiten1 s2.0 S0022316622164783 Mainbesti verawatiNoch keine Bewertungen
- Approaches To Obesity Management: ClinicalperspectivesDokument6 SeitenApproaches To Obesity Management: ClinicalperspectivesSandra CardosoNoch keine Bewertungen
- Artigo Opiniao AlemaDokument6 SeitenArtigo Opiniao Alemacris97Noch keine Bewertungen
- Vegetarian Diets and The Risk of DiabetesDokument6 SeitenVegetarian Diets and The Risk of Diabetesmade dedyNoch keine Bewertungen
- A Systematic Review and Meta-Analysis of Ayurvedic Herbal Preparations For HypercholesterolemiaDokument24 SeitenA Systematic Review and Meta-Analysis of Ayurvedic Herbal Preparations For HypercholesterolemiaSotiris AnagnostopoulosNoch keine Bewertungen
- TMP ABB8Dokument10 SeitenTMP ABB8FrontiersNoch keine Bewertungen
- Defining A Healthy Diet - Evidence For The Role of Contemporary Dietary Patterns in Health and DiseaseDokument15 SeitenDefining A Healthy Diet - Evidence For The Role of Contemporary Dietary Patterns in Health and DiseaseARESS RIPNoch keine Bewertungen
- JCC 20005Dokument10 SeitenJCC 20005Himani PandyaNoch keine Bewertungen
- Conor P. Kerley, 2018.Dokument11 SeitenConor P. Kerley, 2018.MelissaNoch keine Bewertungen
- Anti-Inflammatory Diet To Reduce Mortality Is It Time For A Precision Medicine ApproachDokument3 SeitenAnti-Inflammatory Diet To Reduce Mortality Is It Time For A Precision Medicine ApproachAugusto FuscoNoch keine Bewertungen
- Articulo Dislipidemias 2Dokument16 SeitenArticulo Dislipidemias 2DANIELA CALDERON SAGAHONNoch keine Bewertungen
- Nutrition and Disease: A Mediterranean Diet Is Cost-Effective in Patients With Previous Myocardial InfarctionDokument7 SeitenNutrition and Disease: A Mediterranean Diet Is Cost-Effective in Patients With Previous Myocardial InfarctionRenato CastillaNoch keine Bewertungen
- Nutrients: Ffects of Different Quantities and Qualities ofDokument12 SeitenNutrients: Ffects of Different Quantities and Qualities ofLucas CanaleNoch keine Bewertungen
- Nutrients 09 00848Dokument13 SeitenNutrients 09 00848Ririn Natasia SitinjakNoch keine Bewertungen
- International Journal of Nursing and Health Services (IJNHS)Dokument11 SeitenInternational Journal of Nursing and Health Services (IJNHS)Medianto C.PNoch keine Bewertungen
- Dietary Manipulation in Musculoskeletal Conditions: .R A Y M An@surrey - Ac.ukDokument29 SeitenDietary Manipulation in Musculoskeletal Conditions: .R A Y M An@surrey - Ac.ukbagasNoch keine Bewertungen
- Dietaty Patterns in Stroke Patients in Northwest India: (Journal Study)Dokument3 SeitenDietaty Patterns in Stroke Patients in Northwest India: (Journal Study)Marcus Philip GonzalesNoch keine Bewertungen
- Journal of Hypertension and Management JHM 5 037Dokument10 SeitenJournal of Hypertension and Management JHM 5 037reducdyantaNoch keine Bewertungen
- Hyperlipidemia: Its Management and Induction: Kaushik Et Al.Dokument5 SeitenHyperlipidemia: Its Management and Induction: Kaushik Et Al.mesarraNoch keine Bewertungen
- 营养:疾病预防和治疗Dokument12 Seiten营养:疾病预防和治疗张芬Noch keine Bewertungen
- Farmac ObesidadDokument12 SeitenFarmac ObesidadLeonardo MedinaNoch keine Bewertungen
- Defining A Healthy Diet Evidence For The Role of CDokument15 SeitenDefining A Healthy Diet Evidence For The Role of Canarosli251Noch keine Bewertungen
- Diet and Nutrition in Cancer Survivorship and Palliative CareDokument12 SeitenDiet and Nutrition in Cancer Survivorship and Palliative CareAna Leticia RibeiroNoch keine Bewertungen
- REDALYGDokument8 SeitenREDALYGjoel cedeño SánchezNoch keine Bewertungen
- Nutrients 15 03987 v3Dokument19 SeitenNutrients 15 03987 v3Rosmery SalasNoch keine Bewertungen
- NIH Public Access: A Review of The Hypoglycemic Effects of Five Commonly Used Herbal Food SupplementsDokument22 SeitenNIH Public Access: A Review of The Hypoglycemic Effects of Five Commonly Used Herbal Food SupplementsDaleKadalNoch keine Bewertungen
- Nutrition 411: The Diabetic Foot Ulcer - Can Diet Make A Difference?Dokument4 SeitenNutrition 411: The Diabetic Foot Ulcer - Can Diet Make A Difference?RohmatullahNoch keine Bewertungen
- Nutritional Management and Dietary Guidelines For Cancer CachexiaDokument3 SeitenNutritional Management and Dietary Guidelines For Cancer CachexiaShalah Marie UbaldoNoch keine Bewertungen
- 1 IjahmDokument10 Seiten1 IjahmSeftri SaputraNoch keine Bewertungen
- Lifestyle Modification and Hypertension PreventionDokument6 SeitenLifestyle Modification and Hypertension PreventionFahmi Abdul HaqNoch keine Bewertungen
- Impact of Functional Foods On Prevention of Cardiovascular Disease and DiabetesDokument16 SeitenImpact of Functional Foods On Prevention of Cardiovascular Disease and Diabetesİrem Nur AksoyluNoch keine Bewertungen
- Alasan Ke ManusiaDokument12 SeitenAlasan Ke ManusiaafiwahyuNoch keine Bewertungen
- A Ketogenic Diet As An Adjunct To Cancer Treatment - Cancer Therapy AdvisorDokument4 SeitenA Ketogenic Diet As An Adjunct To Cancer Treatment - Cancer Therapy AdvisorJeffery TaylorNoch keine Bewertungen
- Medical Nutrition Therapy For Hemodialysis PatientsDokument24 SeitenMedical Nutrition Therapy For Hemodialysis Patientsraquelt_65Noch keine Bewertungen
- Omega 3Dokument8 SeitenOmega 3Mireya AlejandraNoch keine Bewertungen
- Lifestyle Modification: Weight Control, Exercise, and Smoking CessationDokument12 SeitenLifestyle Modification: Weight Control, Exercise, and Smoking CessationsenthilNoch keine Bewertungen
- Reviews: Lifestyle Interventions For The Prevention and Treatment of HypertensionDokument25 SeitenReviews: Lifestyle Interventions For The Prevention and Treatment of HypertensionRaul Flores LunaNoch keine Bewertungen
- Nutritional Update For Physicians: Plant-Based DietsDokument6 SeitenNutritional Update For Physicians: Plant-Based DietsAria Marta KornasNoch keine Bewertungen
- Liu (Inter)Dokument13 SeitenLiu (Inter)saifulmangopo123Noch keine Bewertungen
- Intakes of Dietary Fiber, VegetablesDokument7 SeitenIntakes of Dietary Fiber, VegetablesaureliaricidNoch keine Bewertungen
- Do We Need Anti Obesity DrugsDokument13 SeitenDo We Need Anti Obesity DrugsJovan MunjizaNoch keine Bewertungen
- Dickey 2001Dokument8 SeitenDickey 2001Neha RauhilaNoch keine Bewertungen
- 2023 - Enfermedad Cardiovascular y Políticas Dietarias @frelDokument4 Seiten2023 - Enfermedad Cardiovascular y Políticas Dietarias @frelJorge Toshio Yazawa ChaconNoch keine Bewertungen
- 1 s2.0 S0039128X13000901 MainDokument5 Seiten1 s2.0 S0039128X13000901 MainA NNoch keine Bewertungen
- 1 s2.0 S240545771930292XDokument9 Seiten1 s2.0 S240545771930292XprayogarathaNoch keine Bewertungen
- Bio-Flavonoids With Promising Anti-Diabetic Potentials: A Critical SurveyDokument26 SeitenBio-Flavonoids With Promising Anti-Diabetic Potentials: A Critical SurveyKris Natalia ManihurukNoch keine Bewertungen
- The Role of Dietary Supplements During Cancer Therapy1Dokument6 SeitenThe Role of Dietary Supplements During Cancer Therapy1Masna ArahmanNoch keine Bewertungen
- Effects of Using Social Networking Sites in Different La - 2017 - Computers in HDokument8 SeitenEffects of Using Social Networking Sites in Different La - 2017 - Computers in HGabriel AndreescuNoch keine Bewertungen
- Dynamics of Self Control in Egocentric Soc - 2017 - Personality and Individual DDokument7 SeitenDynamics of Self Control in Egocentric Soc - 2017 - Personality and Individual DGabriel AndreescuNoch keine Bewertungen
- European Management Journal: Jordi Paniagua, Pawel Korzynski, Alicia Mas-TurDokument13 SeitenEuropean Management Journal: Jordi Paniagua, Pawel Korzynski, Alicia Mas-TurGabriel AndreescuNoch keine Bewertungen
- Brain and Social Networks Fundamental Building Blo - 2017 - Trends in CognitiveDokument17 SeitenBrain and Social Networks Fundamental Building Blo - 2017 - Trends in CognitiveGabriel AndreescuNoch keine Bewertungen
- Ghid Redactare Lucrare LicentaDokument11 SeitenGhid Redactare Lucrare LicentaGabriel AndreescuNoch keine Bewertungen
- The Severe Hypercholesterolemia Phenotype: Clinical Diagnosis, Management, and Emerging TherapiesDokument13 SeitenThe Severe Hypercholesterolemia Phenotype: Clinical Diagnosis, Management, and Emerging TherapiesAdrian KhomanNoch keine Bewertungen
- Obs FizDokument1 SeiteObs FizGabriel AndreescuNoch keine Bewertungen
- Obs FizDokument1 SeiteObs FizGabriel AndreescuNoch keine Bewertungen
- Obs FizDokument1 SeiteObs FizGabriel AndreescuNoch keine Bewertungen
- Lesson 1 - Intro To Highway EngineeringDokument15 SeitenLesson 1 - Intro To Highway EngineeringSaoirseNoch keine Bewertungen
- AtelectasisDokument37 SeitenAtelectasisSandara ParkNoch keine Bewertungen
- Ventricular Septal DefectDokument8 SeitenVentricular Septal DefectWidelmark FarrelNoch keine Bewertungen
- Nitric AcidDokument7 SeitenNitric AcidKuldeep BhattNoch keine Bewertungen
- Terminologi AnatomiaDokument49 SeitenTerminologi AnatomiaLuluk QurrataNoch keine Bewertungen
- Bhert - EoDokument2 SeitenBhert - EoRose Mae LambanecioNoch keine Bewertungen
- BV Lesson Plan 4Dokument3 SeitenBV Lesson Plan 4api-252119803Noch keine Bewertungen
- Penilaian Akhir TahunDokument4 SeitenPenilaian Akhir TahunRestu Suci UtamiNoch keine Bewertungen
- Join Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsDokument24 SeitenJoin Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsNaveen KumarNoch keine Bewertungen
- Dungeon World ConversionDokument5 SeitenDungeon World ConversionJosephLouisNadeauNoch keine Bewertungen
- Science 9 Q4 SML17 V2Dokument15 SeitenScience 9 Q4 SML17 V2HotdogNoch keine Bewertungen
- Multi-Wing Engineering GuideDokument7 SeitenMulti-Wing Engineering Guidea_salehiNoch keine Bewertungen
- Reaction Paper-RprDokument6 SeitenReaction Paper-Rprapi-543457981Noch keine Bewertungen
- انظمة انذار الحريقDokument78 Seitenانظمة انذار الحريقAhmed AliNoch keine Bewertungen
- Advances of Family Apocynaceae A Review - 2017Dokument30 SeitenAdvances of Family Apocynaceae A Review - 2017Владимир ДружининNoch keine Bewertungen
- Q1. (A) The Diagram Shows A Microphone Being Used To Detect The Output From ADokument10 SeitenQ1. (A) The Diagram Shows A Microphone Being Used To Detect The Output From ASivmi MalishaNoch keine Bewertungen
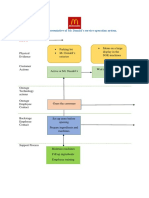
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDokument2 SeitenBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNoch keine Bewertungen
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDokument12 SeitenAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991Noch keine Bewertungen
- Contractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountDokument1 SeiteContractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountusmanaliNoch keine Bewertungen
- Global Talent MonitorDokument30 SeitenGlobal Talent Monitornitinsoni807359Noch keine Bewertungen
- Crime Data Analysis 1Dokument2 SeitenCrime Data Analysis 1kenny laroseNoch keine Bewertungen
- Report On Analysis of TSF Water Samples Using Cyanide PhotometerDokument4 SeitenReport On Analysis of TSF Water Samples Using Cyanide PhotometerEleazar DequiñaNoch keine Bewertungen
- Soil SSCDokument11 SeitenSoil SSCvkjha623477Noch keine Bewertungen
- Valve Material SpecificationDokument397 SeitenValve Material Specificationkaruna34680% (5)
- Paper Specific Instructions:: GATE Chemical Engineering MSQ Paper - 1Dokument11 SeitenPaper Specific Instructions:: GATE Chemical Engineering MSQ Paper - 1Mayank ShelarNoch keine Bewertungen
- Cadorna, Chesca L. - NCPDokument2 SeitenCadorna, Chesca L. - NCPCadorna Chesca LoboNoch keine Bewertungen
- Heteropolyacids FurfuralacetoneDokument12 SeitenHeteropolyacids FurfuralacetonecligcodiNoch keine Bewertungen
- REV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Dokument2 SeitenREV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Bacano CapoeiraNoch keine Bewertungen
- Rooftop Rain Water Harvesting in An Educational CampusDokument9 SeitenRooftop Rain Water Harvesting in An Educational CampusAkshay BoratiNoch keine Bewertungen
- Gendec - Inbound HS-HTNDokument1 SeiteGendec - Inbound HS-HTNKhalidNoch keine Bewertungen
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 4.5 von 5 Sternen4.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Love Yourself, Heal Your Life Workbook (Insight Guide)Von EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Bewertung: 5 von 5 Sternen5/5 (40)
- Summary of Mary Claire Haver's The Galveston DietVon EverandSummary of Mary Claire Haver's The Galveston DietBewertung: 5 von 5 Sternen5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- The End of Craving: Recovering the Lost Wisdom of Eating WellVon EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellBewertung: 4.5 von 5 Sternen4.5/5 (81)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarVon EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarBewertung: 5 von 5 Sternen5/5 (351)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyVon EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNoch keine Bewertungen
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessVon EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessNoch keine Bewertungen
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthVon EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthBewertung: 4 von 5 Sternen4/5 (6)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (411)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeVon EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeBewertung: 4 von 5 Sternen4/5 (3)
- Eat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthVon EverandEat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthBewertung: 2 von 5 Sternen2/5 (1)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouVon EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNoch keine Bewertungen
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainVon EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainBewertung: 3.5 von 5 Sternen3.5/5 (38)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsVon EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsBewertung: 4 von 5 Sternen4/5 (49)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomVon EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomBewertung: 4 von 5 Sternen4/5 (1)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthVon EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNoch keine Bewertungen
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthVon EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthBewertung: 4 von 5 Sternen4/5 (7)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeVon EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeBewertung: 4 von 5 Sternen4/5 (3)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingVon EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingBewertung: 4 von 5 Sternen4/5 (3)
- Molecules of Emotion: Why You Feel the Way You FeelVon EverandMolecules of Emotion: Why You Feel the Way You FeelBewertung: 4 von 5 Sternen4/5 (128)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeVon EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeBewertung: 5 von 5 Sternen5/5 (1)
- The Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoVon EverandThe Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoNoch keine Bewertungen