Das könnte Ihnen auch gefallen
- 400-750 NM AccommodationDokument2 Seiten400-750 NM AccommodationTeves AdrianNoch keine Bewertungen
- 1 - Newman1973Dokument16 Seiten1 - Newman1973Eduardo HernandezNoch keine Bewertungen
- 0 OphthalmologyDokument12 Seiten0 OphthalmologyParsaant SinghNoch keine Bewertungen
- The Eye Is Made Up of THREE LayersDokument2 SeitenThe Eye Is Made Up of THREE LayersMarissa AsimNoch keine Bewertungen
- The Special SensesDokument34 SeitenThe Special SensespuchioNoch keine Bewertungen
- Class01 - 08 Visual Optics IntroductionDokument13 SeitenClass01 - 08 Visual Optics IntroductioncehborrotoNoch keine Bewertungen
- BioPsy 5 - SensationsDokument13 SeitenBioPsy 5 - SensationsTim AroscoNoch keine Bewertungen
- L1 - History and Physical ExaminationDokument22 SeitenL1 - History and Physical ExaminationConger CongerNoch keine Bewertungen
- 27 Physiology of Visual AnalyzerDokument39 Seiten27 Physiology of Visual Analyzersiwap34656Noch keine Bewertungen
- OPTHA 2.1 RETINAL DISORDERS, CHOROID AND VITREOUS - Dr. MarinDokument9 SeitenOPTHA 2.1 RETINAL DISORDERS, CHOROID AND VITREOUS - Dr. MarinPatricia ManaliliNoch keine Bewertungen
- Real Answers in Real Time: Stratus OCTDokument12 SeitenReal Answers in Real Time: Stratus OCTMohammad Abdullah BawtagNoch keine Bewertungen
- Useful For Fixation and FoggingDokument12 SeitenUseful For Fixation and FogginganggastavasthiNoch keine Bewertungen
- Optic Nerve Examination in Glaucoma (Edit)Dokument27 SeitenOptic Nerve Examination in Glaucoma (Edit)mazidahzulfa100% (1)
- Finals Neurologic AssessmentDokument21 SeitenFinals Neurologic Assessmentleih jsNoch keine Bewertungen
- Funduscopy in GlaucomaDokument1 SeiteFunduscopy in Glaucomanadia emildaNoch keine Bewertungen
- L 01 Ocular AnatomyDokument13 SeitenL 01 Ocular Anatomydoni anandaNoch keine Bewertungen
- 5 Assessment and Diagnostic Procedures For Visual and Eye DisordersDokument5 Seiten5 Assessment and Diagnostic Procedures For Visual and Eye DisordersNica EnriquezNoch keine Bewertungen
- OPHTHA 8.0 Neuro Ophthalmology Fundamentals Dr. AtienzaDokument14 SeitenOPHTHA 8.0 Neuro Ophthalmology Fundamentals Dr. AtienzaMaria Gracia YamsonNoch keine Bewertungen
- Blurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocDokument15 SeitenBlurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocRea Dominique CabanillaNoch keine Bewertungen
- 10 - Accommodation & Pupillary Light ReflexDokument46 Seiten10 - Accommodation & Pupillary Light ReflexSugumar YathavanNoch keine Bewertungen
- Fisiologi PenglihatanDokument76 SeitenFisiologi PenglihatanArsyil Ardiman MirwanNoch keine Bewertungen
- Cranial Nerve AssessmentDokument42 SeitenCranial Nerve Assessmentmalik003100% (1)
- Cranialnerveassessmentfinal 140501113414 Phpapp01 PDFDokument42 SeitenCranialnerveassessmentfinal 140501113414 Phpapp01 PDFAlma Baterina100% (1)
- Cranial Nerve AssessmentDokument42 SeitenCranial Nerve AssessmentValeryn Quiman100% (7)
- 2 2 Sensory OrgansDokument27 Seiten2 2 Sensory OrgansKeashi VelzyNoch keine Bewertungen
- Pupillary Pathway, Pupillary Abnormalities, RAPDDokument24 SeitenPupillary Pathway, Pupillary Abnormalities, RAPD015Afeefa N ANoch keine Bewertungen
- From Light To Features: Dr. Sjoerd StuitDokument65 SeitenFrom Light To Features: Dr. Sjoerd StuitsethNoch keine Bewertungen
- 2-Cranial Nerve II Part LecDokument2 Seiten2-Cranial Nerve II Part LecCZARINA TUAZONNoch keine Bewertungen
- Assessment of Neurological SystemDokument26 SeitenAssessment of Neurological SystemBatiao Camille Claire100% (1)
- Refractive Errors ScriptDokument5 SeitenRefractive Errors ScriptSamsam Almarez BacaltosNoch keine Bewertungen
- The Human Brain An Introduction To Its Functional.35Dokument8 SeitenThe Human Brain An Introduction To Its Functional.35Chi Kit ChauNoch keine Bewertungen
- Isolated Abducens Nerve Palsy: Update On Evaluation and DiagnosisDokument1 SeiteIsolated Abducens Nerve Palsy: Update On Evaluation and DiagnosisalecsaNoch keine Bewertungen
- Nerve SonographyDokument11 SeitenNerve SonographysurnameNoch keine Bewertungen
- Retina and Vitreous: OphthalmologyDokument14 SeitenRetina and Vitreous: OphthalmologyPrincess Noreen SavellanoNoch keine Bewertungen
- Physiology of Vision Intraocular Pressure Formation, Circulation & Drainage of Aqueous HumorDokument15 SeitenPhysiology of Vision Intraocular Pressure Formation, Circulation & Drainage of Aqueous HumorRida ArifNoch keine Bewertungen
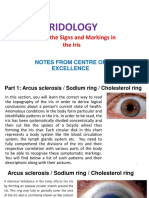
- Iridology-Signs and MarkingsDokument14 SeitenIridology-Signs and MarkingsforangNoch keine Bewertungen
- ANAT204 Vision 2011Dokument18 SeitenANAT204 Vision 2011freaky-mario3327Noch keine Bewertungen
- Orbital Apex Syndrome. A ReviewDokument10 SeitenOrbital Apex Syndrome. A ReviewAndrés Faúndez TeránNoch keine Bewertungen
- Case RRDDokument56 SeitenCase RRDRana AhmedNoch keine Bewertungen
- Eye 2Dokument5 SeitenEye 2Nadia AbdurasidNoch keine Bewertungen
- Primary Visual Pathway: LIFE3082 Sensational NeuroscienceDokument27 SeitenPrimary Visual Pathway: LIFE3082 Sensational NeuroscienceAngkelova ChristinaNoch keine Bewertungen
- Lens and Cataract - Dr. Angbue-Te (2023)Dokument4 SeitenLens and Cataract - Dr. Angbue-Te (2023)Patricia ManaliliNoch keine Bewertungen
- Class 4Dokument12 SeitenClass 4PS SuryaNoch keine Bewertungen
- Motor Control - Visual SystemDokument32 SeitenMotor Control - Visual SystemJanani IyerNoch keine Bewertungen
- Part1 - Eye - DV (7 Files Merged)Dokument127 SeitenPart1 - Eye - DV (7 Files Merged)Matthew MalekNoch keine Bewertungen
- Visual PathwayDokument63 SeitenVisual Pathwaysenny chapagainNoch keine Bewertungen
- 12-2 - Fri - vision-hearing-EQDokument13 Seiten12-2 - Fri - vision-hearing-EQTyler DeanNoch keine Bewertungen
- SGD Case Bustamante Patricia MaricDokument30 SeitenSGD Case Bustamante Patricia MaricJewelNoch keine Bewertungen
- Cranial Nerves PDFDokument8 SeitenCranial Nerves PDFKimberlie HibayaNoch keine Bewertungen
- Pemeriksaan Lapang Pandangan AYUDokument101 SeitenPemeriksaan Lapang Pandangan AYUGlaucoma UnhasNoch keine Bewertungen
- Error of RefractionDokument3 SeitenError of RefractionMargot SanchezNoch keine Bewertungen
- ED II Lens Camerae Bulbivitrous Body Accomodation TZSDokument25 SeitenED II Lens Camerae Bulbivitrous Body Accomodation TZSBojanaNoch keine Bewertungen
- Assessment of Visual and Auditory Sy: st0msDokument28 SeitenAssessment of Visual and Auditory Sy: st0msSomyee PachuauNoch keine Bewertungen
- Journal Article OA PDFDokument6 SeitenJournal Article OA PDFPutu 'yayuk' Widyani WiradiraniNoch keine Bewertungen
- Specific Objectives Notes Practical: Section ADokument14 SeitenSpecific Objectives Notes Practical: Section AaWDwaDNoch keine Bewertungen
- Bloqueos Miembro SuperiorDokument1 SeiteBloqueos Miembro SuperiorpimpollopittNoch keine Bewertungen
- ED Slit Lamp ExaminationDokument23 SeitenED Slit Lamp ExaminationNirmalie RupasingheNoch keine Bewertungen
- NeuroophthalmologyDokument4 SeitenNeuroophthalmologysarguss14100% (2)
- Oculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsVon EverandOculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNoch keine Bewertungen
- Transmitters in the Visual ProcessVon EverandTransmitters in the Visual ProcessS.L. BontingNoch keine Bewertungen
- RC0853 Topical Antibiotics For Infected Wounds Final PDFDokument20 SeitenRC0853 Topical Antibiotics For Infected Wounds Final PDFChristine Yohana SianturiNoch keine Bewertungen
- Ciu296Dokument43 SeitenCiu296Christine Yohana SianturiNoch keine Bewertungen
- RC0853 Topical Antibiotics For Infected Wounds Final PDFDokument20 SeitenRC0853 Topical Antibiotics For Infected Wounds Final PDFChristine Yohana SianturiNoch keine Bewertungen
- Local Wound Care and Topical Management of Hidradenitis SupurativaDokument7 SeitenLocal Wound Care and Topical Management of Hidradenitis SupurativaChristine Yohana SianturiNoch keine Bewertungen
- RC0853 Topical Antibiotics For Infected Wounds Final PDFDokument20 SeitenRC0853 Topical Antibiotics For Infected Wounds Final PDFChristine Yohana SianturiNoch keine Bewertungen
- Flowchart PKTCRDDokument2 SeitenFlowchart PKTCRDChristine Yohana SianturiNoch keine Bewertungen
- Family Wellness Plan Keluarga Bapak GunawanDokument2 SeitenFamily Wellness Plan Keluarga Bapak GunawanChristine Yohana SianturiNoch keine Bewertungen
- (Read) Ijcn-9-046 PDFDokument7 Seiten(Read) Ijcn-9-046 PDFChristine Yohana SianturiNoch keine Bewertungen
- Five DebatesDokument37 SeitenFive DebatesIffi ButtNoch keine Bewertungen
- Cshperspectmed BEP A022426Dokument18 SeitenCshperspectmed BEP A022426Ahmad FahroziNoch keine Bewertungen
- (Read) Ijcn-9-046 PDFDokument7 Seiten(Read) Ijcn-9-046 PDFChristine Yohana SianturiNoch keine Bewertungen
- PDZVBB - 18 Jun 2018Dokument12 SeitenPDZVBB - 18 Jun 2018Christine Yohana SianturiNoch keine Bewertungen
- Cshperspectmed BEP A022426Dokument18 SeitenCshperspectmed BEP A022426Ahmad FahroziNoch keine Bewertungen
- Jurnal Bahasa InggrisDokument8 SeitenJurnal Bahasa InggrisChristine Yohana SianturiNoch keine Bewertungen
- Salmonella EnteriticaDokument23 SeitenSalmonella EnteriticaChristine Yohana SianturiNoch keine Bewertungen
- SDLR 2016 (Penelitian)Dokument8 SeitenSDLR 2016 (Penelitian)Christine Yohana SianturiNoch keine Bewertungen
- SDLR 2016 (Penelitian)Dokument8 SeitenSDLR 2016 (Penelitian)Christine Yohana SianturiNoch keine Bewertungen
- Current Concepts in The Diagnosis and Treatment of Typhoid FeverDokument5 SeitenCurrent Concepts in The Diagnosis and Treatment of Typhoid FeverMohamed OmerNoch keine Bewertungen
- Breathing Exercise Thomas 2014Dokument12 SeitenBreathing Exercise Thomas 2014Christine Yohana SianturiNoch keine Bewertungen
- Hasil StatistikDokument8 SeitenHasil StatistikChristine Yohana SianturiNoch keine Bewertungen
- A Comparative Study of Widal Test With Blood Culture in The Diagnosis of Typhoid Fever in Febrile PatientsDokument6 SeitenA Comparative Study of Widal Test With Blood Culture in The Diagnosis of Typhoid Fever in Febrile PatientsHana AgustianaNoch keine Bewertungen
- The Lucid Interval Associated With Epidural Bleeding: Evolving UnderstandingDokument7 SeitenThe Lucid Interval Associated With Epidural Bleeding: Evolving UnderstandingyosiaputraNoch keine Bewertungen
- Weiner - UltrasoundDokument55 SeitenWeiner - UltrasoundChristine Yohana SianturiNoch keine Bewertungen
- Hasil StatistikDokument8 SeitenHasil StatistikChristine Yohana SianturiNoch keine Bewertungen
- Comparative Widal and Blooc Culture 2014Dokument19 SeitenComparative Widal and Blooc Culture 2014Christine Yohana SianturiNoch keine Bewertungen
- Daftar Isi Sampai Kata PengantarDokument2 SeitenDaftar Isi Sampai Kata PengantarChristine Yohana SianturiNoch keine Bewertungen
- PDZVBB - 18 Jun 2018 PDFDokument1 SeitePDZVBB - 18 Jun 2018 PDFChristine Yohana SianturiNoch keine Bewertungen
- 163full PDFDokument30 Seiten163full PDFChristine Yohana SianturiNoch keine Bewertungen
- PDZVBB - 18 Jun 2018 PDFDokument1 SeitePDZVBB - 18 Jun 2018 PDFChristine Yohana SianturiNoch keine Bewertungen
- Myopia Control: A Review: Jeffrey J. WallineDokument6 SeitenMyopia Control: A Review: Jeffrey J. WallineChristine Yohana SianturiNoch keine Bewertungen
- PET Formal Letter SamplesDokument7 SeitenPET Formal Letter SamplesLe Anh ThuNoch keine Bewertungen
- English Literature Coursework Aqa GcseDokument6 SeitenEnglish Literature Coursework Aqa Gcsef5d17e05100% (2)
- Series R: 3 Piece Ball Valves With Integrated Handle DN8 - DN50 Butt Weld, Threaded, Socket Weld and Flanged VersionDokument2 SeitenSeries R: 3 Piece Ball Valves With Integrated Handle DN8 - DN50 Butt Weld, Threaded, Socket Weld and Flanged VersionАртем КосовNoch keine Bewertungen
- I. Matching Type. Write Letters Only. (10pts) : Adamson University Computer Literacy 2 Prelim ExamDokument2 SeitenI. Matching Type. Write Letters Only. (10pts) : Adamson University Computer Literacy 2 Prelim ExamFerrolinoLouieNoch keine Bewertungen
- Amazon Tax Information InterviewDokument2 SeitenAmazon Tax Information Interviewasad nNoch keine Bewertungen
- Smarajit Ghosh - Control Systems - Theory and Applications-Pearson (2006) PDFDokument629 SeitenSmarajit Ghosh - Control Systems - Theory and Applications-Pearson (2006) PDFaggarwalakanksha100% (2)
- DWDMDokument41 SeitenDWDMKarthik KompelliNoch keine Bewertungen
- Fuel Injection PDFDokument11 SeitenFuel Injection PDFscaniaNoch keine Bewertungen
- Developing Sui-Generis System For The Protection of Trade Secret in India: An Analytical StudyDokument8 SeitenDeveloping Sui-Generis System For The Protection of Trade Secret in India: An Analytical StudyVEENA T NNoch keine Bewertungen
- UGC NET Paper I PreviousDokument16 SeitenUGC NET Paper I PreviousKirran Khumar GollaNoch keine Bewertungen
- Fish Siomai RecipeDokument12 SeitenFish Siomai RecipeRhyz Mareschal DongonNoch keine Bewertungen
- Sample Heat Sheets June 2007Dokument63 SeitenSample Heat Sheets June 2007Nesuui MontejoNoch keine Bewertungen
- GRADE 1 MUSIC Week 1 Learning PacketsDokument16 SeitenGRADE 1 MUSIC Week 1 Learning PacketsQuennie Rose EderNoch keine Bewertungen
- BCSS Sec Unit 1 Listening and Speaking SkillsDokument16 SeitenBCSS Sec Unit 1 Listening and Speaking Skillsjiny benNoch keine Bewertungen
- W1 - V1 MultipleWorksheets SolnDokument3 SeitenW1 - V1 MultipleWorksheets SolnAKHIL RAJ SNoch keine Bewertungen
- Study of Bond Properties of Concrete Utilizing Fly Ash, Marble and Granite PowderDokument3 SeitenStudy of Bond Properties of Concrete Utilizing Fly Ash, Marble and Granite PowderLegaldevil LlabsNoch keine Bewertungen
- Pinto pm5 Tif 02Dokument24 SeitenPinto pm5 Tif 02Salem BawazirNoch keine Bewertungen
- CHAPTER I KyleDokument13 SeitenCHAPTER I KyleCresiel Pontijon100% (1)
- What Is A Timer?Dokument12 SeitenWhat Is A Timer?Hemraj Singh Rautela100% (1)
- Role of ACT, S & WHO Guidlines For The Treatment of MalariaDokument34 SeitenRole of ACT, S & WHO Guidlines For The Treatment of MalariasalmanNoch keine Bewertungen
- Inkolo Namasiko Kuyamakha Umuntu - Brainly - inDokument1 SeiteInkolo Namasiko Kuyamakha Umuntu - Brainly - inxqxfkqpy5qNoch keine Bewertungen
- Skin Care Creams, Lotions and Gels For Cosmetic Use - SpecificationDokument33 SeitenSkin Care Creams, Lotions and Gels For Cosmetic Use - SpecificationJona Phie Montero NdtcnursingNoch keine Bewertungen
- Plant Gardening AerationDokument4 SeitenPlant Gardening Aerationut.testbox7243Noch keine Bewertungen
- Student's T DistributionDokument6 SeitenStudent's T DistributionNur AliaNoch keine Bewertungen
- Antonov 225 - The Largest - Airliner in The WorldDokument63 SeitenAntonov 225 - The Largest - Airliner in The WorldFridayFunStuffNoch keine Bewertungen
- Business Maths Chapter 5Dokument9 SeitenBusiness Maths Chapter 5鄭仲抗Noch keine Bewertungen
- Fabrication Daily Progress: No DescriptionDokument4 SeitenFabrication Daily Progress: No DescriptionAris PurniawanNoch keine Bewertungen
- Psi Engines Product Sheet PDFDokument2 SeitenPsi Engines Product Sheet PDFDaniel DelgadoNoch keine Bewertungen
- Bangalore Escorts Services - Riya ShettyDokument11 SeitenBangalore Escorts Services - Riya ShettyRiya ShettyNoch keine Bewertungen
- Writofsummons ForrevisionpurposesonlyDokument7 SeitenWritofsummons ForrevisionpurposesonlyNuur KhaliilahNoch keine Bewertungen