Das könnte Ihnen auch gefallen
- Comprehensive Handbook of Clinical Health PsychologyVon EverandComprehensive Handbook of Clinical Health PsychologyBret A BoyerNoch keine Bewertungen
- Psychiatric Diagnosis: Challenges and ProspectsVon EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumBewertung: 5 von 5 Sternen5/5 (1)
- Counseling Vs Clinical PsychologistDokument2 SeitenCounseling Vs Clinical PsychologistOsvaldo González CartagenaNoch keine Bewertungen
- Clinical PsychologistDokument1 SeiteClinical PsychologistlackbarryNoch keine Bewertungen
- Arizona Clinical Interview Rating ScaleDokument5 SeitenArizona Clinical Interview Rating ScaleArbnor Kica100% (1)
- PSYCH - PsychosomaticdelasalleDokument58 SeitenPSYCH - Psychosomaticdelasalleapi-3856051100% (1)
- Psychology Talks 2011 - DR Gitanjali (NUH)Dokument31 SeitenPsychology Talks 2011 - DR Gitanjali (NUH)nuspsycheNoch keine Bewertungen
- Youngmee Kim - Gender in Psycho-Oncology (2018, Oxford University Press, USA)Dokument263 SeitenYoungmee Kim - Gender in Psycho-Oncology (2018, Oxford University Press, USA)Dian Oktaria SafitriNoch keine Bewertungen
- Cigarette Smoking in Patients With Schizophrenia in Turkey Relationships To Psychopatology, Soci-Demographic and Clinical Characteristics PDFDokument9 SeitenCigarette Smoking in Patients With Schizophrenia in Turkey Relationships To Psychopatology, Soci-Demographic and Clinical Characteristics PDFEmiNoch keine Bewertungen
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Dokument4 SeitenPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNoch keine Bewertungen
- Professional Competency Assessment 1Dokument19 SeitenProfessional Competency Assessment 1Bruce MannNoch keine Bewertungen
- Secondary Traumatic Stress Scale (STSS)Dokument1 SeiteSecondary Traumatic Stress Scale (STSS)MilosNoch keine Bewertungen
- The Use of Mobile Device Application For Assessing Pain Pattern in Veteran Patients With Mild Traumatic Brain Injury Related HeadachesDokument27 SeitenThe Use of Mobile Device Application For Assessing Pain Pattern in Veteran Patients With Mild Traumatic Brain Injury Related Headachesapi-529388510Noch keine Bewertungen
- Psychologist or School Psychologist or Therapist or CounselorDokument2 SeitenPsychologist or School Psychologist or Therapist or Counselorapi-79222085Noch keine Bewertungen
- Psychological Assessment ReportDokument3 SeitenPsychological Assessment ReportmobeenNoch keine Bewertungen
- 1999 Aversion Therapy-BEDokument6 Seiten1999 Aversion Therapy-BEprabhaNoch keine Bewertungen
- 4 - Guidelines For HIV Care and Treatment in Infants and ChildrenDokument136 Seiten4 - Guidelines For HIV Care and Treatment in Infants and Childreniman_kundu2007756100% (1)
- The Psychology of Gender: PSYC-362-DL1 Taught By: Jason Feinberg Welcome!Dokument58 SeitenThe Psychology of Gender: PSYC-362-DL1 Taught By: Jason Feinberg Welcome!uhhhhNoch keine Bewertungen
- The Extended Bio-Psycho-Social Model: A Few Evidences of Its EffectivenessDokument3 SeitenThe Extended Bio-Psycho-Social Model: A Few Evidences of Its EffectivenessHemant KumarNoch keine Bewertungen
- SDQDokument3 SeitenSDQSarah AzminNoch keine Bewertungen
- PSC-17 Scoring Instructions PDFDokument1 SeitePSC-17 Scoring Instructions PDFMayang Sukma SatriaNoch keine Bewertungen
- Evaluación de Abuso SexualDokument14 SeitenEvaluación de Abuso SexualLaura Sánchez RodríguezNoch keine Bewertungen
- 8 Ways To Control StressDokument2 Seiten8 Ways To Control Stressstcyrjr510Noch keine Bewertungen
- Module 3 Biochemistry of The BrainDokument12 SeitenModule 3 Biochemistry of The BrainSakshi Jauhari100% (1)
- Clinical Application of The DSM-5 in Private CounselingDokument15 SeitenClinical Application of The DSM-5 in Private CounselingRoss CameronNoch keine Bewertungen
- Mill Shul Bert Williams 2012Dokument25 SeitenMill Shul Bert Williams 2012AdityaTirtakusumaNoch keine Bewertungen
- WHOQOL-BREF With Scoring Instructions - Updated 01-10-14Dokument12 SeitenWHOQOL-BREF With Scoring Instructions - Updated 01-10-14Sean Cho0% (1)
- Response Set (Psychological Perspective)Dokument15 SeitenResponse Set (Psychological Perspective)MacxieNoch keine Bewertungen
- QLD Drug Price ListDokument1 SeiteQLD Drug Price ListMayNoch keine Bewertungen
- Biopsychosocial ModelDokument5 SeitenBiopsychosocial ModelElysium Minds100% (1)
- Perinatal Anxiety Screening ScaleDokument8 SeitenPerinatal Anxiety Screening ScaleAprillia RNoch keine Bewertungen
- H.5.1 Antipsychotics PowerPoint 2016Dokument55 SeitenH.5.1 Antipsychotics PowerPoint 2016Ptrc Lbr LpNoch keine Bewertungen
- Childhood Depression Presentation OutlineDokument7 SeitenChildhood Depression Presentation Outlineapi-290018716Noch keine Bewertungen
- Final ThesisDokument120 SeitenFinal ThesisSingh SoniyaNoch keine Bewertungen
- School-Based Intervention Relaxation and Guided Imagery For Students With Asthma and Anxiety DisorderDokument19 SeitenSchool-Based Intervention Relaxation and Guided Imagery For Students With Asthma and Anxiety DisorderWidiastuti PajariniNoch keine Bewertungen
- Helping Men Recover: Addiction, Males, and The Missing PeaceDokument8 SeitenHelping Men Recover: Addiction, Males, and The Missing Peacetadcp100% (1)
- ETZI - 2014 - The Psychodynamic Diagnostic Manual M AxisDokument16 SeitenETZI - 2014 - The Psychodynamic Diagnostic Manual M AxisLoratadinaNoch keine Bewertungen
- An Overview of The Interview ProcessDokument6 SeitenAn Overview of The Interview ProcessLaura ZarrateNoch keine Bewertungen
- The EMDR Therapy Butter y Hug Method For Self-Administer Bilateral StimulationDokument8 SeitenThe EMDR Therapy Butter y Hug Method For Self-Administer Bilateral StimulationYulian Dwi Putra FJNoch keine Bewertungen
- CatDokument12 SeitenCatnini345Noch keine Bewertungen
- Tourette Syndrome Research PaperDokument7 SeitenTourette Syndrome Research PaperAtme SmileNoch keine Bewertungen
- Assessment Scale For DeliriumDokument13 SeitenAssessment Scale For DeliriumPutu Agus GrantikaNoch keine Bewertungen
- Functionalism: American Psychology Takes HoldDokument17 SeitenFunctionalism: American Psychology Takes HoldTehran DavisNoch keine Bewertungen
- Tolman Theory of LearningDokument4 SeitenTolman Theory of LearningBigyan BasaulaNoch keine Bewertungen
- Tourette's SyndromeDokument31 SeitenTourette's SyndromeGhadeer AlomariNoch keine Bewertungen
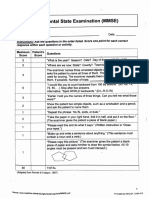
- Mini-Mental State Examination (MMSE)Dokument3 SeitenMini-Mental State Examination (MMSE)Prescilla San PedroNoch keine Bewertungen
- CDI Patient VersionDokument9 SeitenCDI Patient VersionalotfyaNoch keine Bewertungen
- Clinical Case HistoryDokument5 SeitenClinical Case HistoryMahrukhNoch keine Bewertungen
- Andreasen 1989Dokument4 SeitenAndreasen 1989RaquelNoch keine Bewertungen
- Cultural Issue Schizophrenia IndiaDokument58 SeitenCultural Issue Schizophrenia IndiaSam InvincibleNoch keine Bewertungen
- Dummy ReportDokument29 SeitenDummy ReportnaquiahoNoch keine Bewertungen
- 16PF BibDokument10 Seiten16PF BibdocagunsNoch keine Bewertungen
- Bariatric Surgery BH Grand RoundsDokument39 SeitenBariatric Surgery BH Grand Roundsapi-440514424Noch keine Bewertungen
- Literature ReviewDokument9 SeitenLiterature ReviewCarlee ChynowethNoch keine Bewertungen
- Personality Disorders PDFDokument414 SeitenPersonality Disorders PDFLorina SanduNoch keine Bewertungen
- CV For Dr. Keely KolmesDokument9 SeitenCV For Dr. Keely KolmesdrkkolmesNoch keine Bewertungen
- Dr. Jagdeo Survival ManualDokument16 SeitenDr. Jagdeo Survival ManualAli BabaNoch keine Bewertungen
- Competency MappingDokument20 SeitenCompetency MappingJagan Mba0% (1)
- QS: Social Exchange Theory: FoundersDokument2 SeitenQS: Social Exchange Theory: FounderssoulxpressNoch keine Bewertungen
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenVon EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNoch keine Bewertungen
- David Gordon - Phoenix - Therapeutic Patterns of Milton H. EricksonDokument203 SeitenDavid Gordon - Phoenix - Therapeutic Patterns of Milton H. EricksonNora Grigoruta100% (9)
- An Investigation of Health Anxiety in FamiliesDokument12 SeitenAn Investigation of Health Anxiety in FamiliesAndreea NicolaeNoch keine Bewertungen
- 382 Full PDFDokument22 Seiten382 Full PDFAndreea NicolaeNoch keine Bewertungen
- 555 Full PDFDokument21 Seiten555 Full PDFAndreea NicolaeNoch keine Bewertungen
- Animalele - Material Terapie ABADokument17 SeitenAnimalele - Material Terapie ABAAndreea NicolaeNoch keine Bewertungen
- Time Limited Psychotherapy PDFDokument52 SeitenTime Limited Psychotherapy PDFlara_2772Noch keine Bewertungen
- Behavioral Therapy For Anxiety DisordersDokument18 SeitenBehavioral Therapy For Anxiety DisordersAndreea NicolaeNoch keine Bewertungen
- 3 Full PDFDokument21 Seiten3 Full PDFAndreea NicolaeNoch keine Bewertungen
- A Time-Series Study of The Treatment of Panic DisorderDokument21 SeitenA Time-Series Study of The Treatment of Panic Disordermetramor8745Noch keine Bewertungen
- Behavioral Therapy For Anxiety DisordersDokument18 SeitenBehavioral Therapy For Anxiety DisordersAndreea NicolaeNoch keine Bewertungen
- Oppositional Defiant DisorderDokument13 SeitenOppositional Defiant DisorderAndreea NicolaeNoch keine Bewertungen
- Behavioral Therapy For Anxiety DisordersDokument18 SeitenBehavioral Therapy For Anxiety DisordersAndreea NicolaeNoch keine Bewertungen
- Don't Kick Me OutDokument14 SeitenDon't Kick Me OutAndreea NicolaeNoch keine Bewertungen
- Cognitive InterventionDokument13 SeitenCognitive InterventionAndreea NicolaeNoch keine Bewertungen
- The Five Therapeutic RelationshipsDokument16 SeitenThe Five Therapeutic RelationshipsAndreea Nicolae100% (2)
- Treating Depression in Prison Nursing HomeDokument21 SeitenTreating Depression in Prison Nursing HomeAndreea NicolaeNoch keine Bewertungen
- Internet-Related Psychopathology Clinical Phenotypes and PerspectivesDokument138 SeitenInternet-Related Psychopathology Clinical Phenotypes and PerspectivesAndreea NicolaeNoch keine Bewertungen
- Behavioral Activation As An Intervention For Coexistent Depressive and Anxiety SymptomsDokument13 SeitenBehavioral Activation As An Intervention For Coexistent Depressive and Anxiety SymptomsAndreea NicolaeNoch keine Bewertungen
- Relation ASD - ADHDDokument16 SeitenRelation ASD - ADHDAndreea NicolaeNoch keine Bewertungen
- RADDokument25 SeitenRADAndreea NicolaeNoch keine Bewertungen
- Assessment and Behavioral Treatment of Selective MutismDokument22 SeitenAssessment and Behavioral Treatment of Selective MutismAndreea NicolaeNoch keine Bewertungen
- The Use of Homework Success For A Child With Attention-Deficit/ Hyperactivity Disorder, Predominantly Inattentive TypeDokument14 SeitenThe Use of Homework Success For A Child With Attention-Deficit/ Hyperactivity Disorder, Predominantly Inattentive TypeAndreea NicolaeNoch keine Bewertungen
- Behavioral Therapy For Anxiety DisordersDokument18 SeitenBehavioral Therapy For Anxiety DisordersAndreea NicolaeNoch keine Bewertungen
- Trating Food Refusal in Adolescent With Asperger's DisorderDokument14 SeitenTrating Food Refusal in Adolescent With Asperger's DisorderAndreea NicolaeNoch keine Bewertungen
- Therapist As Trauma SurvivorsDokument16 SeitenTherapist As Trauma SurvivorsAndreea NicolaeNoch keine Bewertungen
- Behavioral Therapy For Anxiety DisordersDokument18 SeitenBehavioral Therapy For Anxiety DisordersAndreea NicolaeNoch keine Bewertungen
- The Role of Attention - ASDDokument13 SeitenThe Role of Attention - ASDAndreea NicolaeNoch keine Bewertungen
- The Role of Attention - ASDDokument13 SeitenThe Role of Attention - ASDAndreea NicolaeNoch keine Bewertungen
- 9 Feeding Therapy in A Child With Autistic DisorderDokument12 Seiten9 Feeding Therapy in A Child With Autistic DisorderArden AriandaNoch keine Bewertungen
- Immunity and Vaccines As Biology Answers AQA OCR EdexcelDokument3 SeitenImmunity and Vaccines As Biology Answers AQA OCR EdexcelShela HuangNoch keine Bewertungen
- Medical Record Book Design With Services ListDokument3 SeitenMedical Record Book Design With Services ListNANTHA KUMARANNoch keine Bewertungen
- Fistula in AnoDokument17 SeitenFistula in Anoapi-216828341Noch keine Bewertungen
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDokument7 SeitenRajiv Gandhi University of Health Sciences Bangalore, KarnatakaWirawanSiregarNoch keine Bewertungen
- Letter: Targeting The CBM Complex Causes T Cells To Prime Tumours For Immune Checkpoint TherapyDokument24 SeitenLetter: Targeting The CBM Complex Causes T Cells To Prime Tumours For Immune Checkpoint TherapyZUNENoch keine Bewertungen
- Evnt ASCODokument40 SeitenEvnt ASCOChristopher Praveen KumarNoch keine Bewertungen
- CytomegalovirusDokument33 SeitenCytomegalovirusAnggi Tridinanti PutriNoch keine Bewertungen
- ENTDokument17 SeitenENTNavya ThomasNoch keine Bewertungen
- Spirulina - LatestDokument14 SeitenSpirulina - Latestsenthilswamy_mNoch keine Bewertungen
- Cancer Incidence Report 2020Dokument98 SeitenCancer Incidence Report 2020بسام سالمNoch keine Bewertungen
- Abdominal ExaminationDokument12 SeitenAbdominal ExaminationMukhtar Ahmed100% (1)
- Diffuse Idiopathic Skeletal Hyperostosis (DISH) - StatPearls - NCBI BookshelfDokument7 SeitenDiffuse Idiopathic Skeletal Hyperostosis (DISH) - StatPearls - NCBI BookshelfDavid Ithu AgkhuNoch keine Bewertungen
- Clinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesDokument27 SeitenClinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesradhiinathahirNoch keine Bewertungen
- The Treatment of Cancer With Chinese MedicineDokument6 SeitenThe Treatment of Cancer With Chinese Medicinenepretip100% (2)
- ConjectivaDokument34 SeitenConjectivaIrfan ParakkotNoch keine Bewertungen
- Facit F IndiceDokument5 SeitenFacit F IndiceadolforomeroNoch keine Bewertungen
- Mapeh EssayDokument1 SeiteMapeh EssayJairon BariuanNoch keine Bewertungen
- Haidar Abdul-Muhsin M.D., Vipul Patel M.D. (Auth.), Keith Chae Kim (Eds.) - Robotics in General Surgery-Springer-Verlag New York (2014)Dokument496 SeitenHaidar Abdul-Muhsin M.D., Vipul Patel M.D. (Auth.), Keith Chae Kim (Eds.) - Robotics in General Surgery-Springer-Verlag New York (2014)Bogdan Trandafir100% (1)
- Urological RefferalDokument12 SeitenUrological Refferalmichelle octavianiNoch keine Bewertungen
- Medical AbbreviationDokument76 SeitenMedical AbbreviationNajwa AbdullahNoch keine Bewertungen
- Feature and Sports WritingDokument27 SeitenFeature and Sports WritingJoemar Furigay100% (1)
- History, Examination and Treatment PlaningDokument78 SeitenHistory, Examination and Treatment PlaningShintia HawariNoch keine Bewertungen
- NCP For COLON Cancer PatientDokument4 SeitenNCP For COLON Cancer PatientCarolina Tardecilla100% (1)
- Breast Cancer, Version 3.2020: NCCN Clinical Practice Guidelines in OncologyDokument27 SeitenBreast Cancer, Version 3.2020: NCCN Clinical Practice Guidelines in OncologyHaidzar FNoch keine Bewertungen
- Bacillus Clausii ErcefloraDokument1 SeiteBacillus Clausii ErcefloraCezhille BattadNoch keine Bewertungen
- Cures For TinnitusDokument9 SeitenCures For TinnitusBob Skins100% (2)
- Obesity Case StudyDokument4 SeitenObesity Case Studydsaitta108Noch keine Bewertungen
- Nonoperative Proximal Humeus FractureDokument20 SeitenNonoperative Proximal Humeus FractureLuka DamjanovicNoch keine Bewertungen
- CS ShockDokument5 SeitenCS ShockJuliusSerdeñaTrapal0% (5)
- Ipr F300 Re V12.0Dokument6 SeitenIpr F300 Re V12.0gtmlpatelNoch keine Bewertungen