Das könnte Ihnen auch gefallen
- Guia Hipertension Viii 2014Dokument6 SeitenGuia Hipertension Viii 2014Edgar G RoblesNoch keine Bewertungen
- Amlodipine - Drug Information - UpToDateDokument9 SeitenAmlodipine - Drug Information - UpToDateBárbaraNoch keine Bewertungen
- Managing Heart Failure with Drug TherapyDokument8 SeitenManaging Heart Failure with Drug TherapyAbdallahMousaNoch keine Bewertungen
- A Case of Hypertension in Diabetes This Case Study Aims ToDokument4 SeitenA Case of Hypertension in Diabetes This Case Study Aims Towalit1101 mukrinin100% (1)
- Hypertension: Increase in Blood PressureDokument29 SeitenHypertension: Increase in Blood PressureKeesha Mae AnteNoch keine Bewertungen
- Management of HypertensionDokument19 SeitenManagement of HypertensionChandana RajuNoch keine Bewertungen
- Oleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Dokument40 SeitenOleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Mbenk NjoeNoch keine Bewertungen
- JNC 8 Hypertension Guidelines SimplifiedDokument5 SeitenJNC 8 Hypertension Guidelines SimplifiedAkang Eko Cuman BeginiNoch keine Bewertungen
- Chapter 2 - A - III Hypertension TreatmentDokument37 SeitenChapter 2 - A - III Hypertension TreatmentEmmaNoch keine Bewertungen
- JNC 8 Hypertension Guideline ChangesDokument5 SeitenJNC 8 Hypertension Guideline ChangesdicksonNoch keine Bewertungen
- JNC 8 Hypertension Guidelines Simplify Treatment GoalsDokument6 SeitenJNC 8 Hypertension Guidelines Simplify Treatment GoalsThebounc3Noch keine Bewertungen
- ACE InhibitorsDokument26 SeitenACE Inhibitorsali mohammedNoch keine Bewertungen
- Hypertension: 1-Hypertension Is Defined As (BP)Dokument37 SeitenHypertension: 1-Hypertension Is Defined As (BP)hussein alnasryNoch keine Bewertungen
- Aliskiren and Enalapril in Heart FailureDokument43 SeitenAliskiren and Enalapril in Heart FailureKishor K AdhikariNoch keine Bewertungen
- Hypertension Guideline SummaryDokument12 SeitenHypertension Guideline Summaryمصطفى ابراهيم سعيدNoch keine Bewertungen
- Meds Affecting Blood PressureDokument5 SeitenMeds Affecting Blood PressuremikiNoch keine Bewertungen
- Captopril Pharmacological Properties and UsesDokument13 SeitenCaptopril Pharmacological Properties and UsesputrinadNoch keine Bewertungen
- Lec 3Dokument12 SeitenLec 3Sajjad FalahNoch keine Bewertungen
- Qualitative and Quantitative Formula Aprovel 75 MG Tablets Aprovel 150 MG Tablets Aprovel 300 MG TabletsDokument4 SeitenQualitative and Quantitative Formula Aprovel 75 MG Tablets Aprovel 150 MG Tablets Aprovel 300 MG TabletskatiaelleryNoch keine Bewertungen
- The JNC 8 Hipertensi Pedoman TerbaruDokument6 SeitenThe JNC 8 Hipertensi Pedoman TerbaruMuLyana SariiNoch keine Bewertungen
- Captopril Drug Study for Congestive Heart FailureDokument8 SeitenCaptopril Drug Study for Congestive Heart FailureMae Therese B. MAGNONoch keine Bewertungen
- Hypertension Guidelines 2014: Jason A. Smith, DO Associated Cardiovascular Consultants at Lourdes Cardiology ServicesDokument33 SeitenHypertension Guidelines 2014: Jason A. Smith, DO Associated Cardiovascular Consultants at Lourdes Cardiology ServicesRido MaulanaNoch keine Bewertungen
- Aki and CKD Therapy 2021Dokument46 SeitenAki and CKD Therapy 2021Alfathri YunediNoch keine Bewertungen
- Drug StudyDokument9 SeitenDrug StudyEzshkha OngueNoch keine Bewertungen
- Enalapril: Indications and DosageDokument18 SeitenEnalapril: Indications and Dosageshahera rosdiNoch keine Bewertungen
- Atacand 4 MG, 8 MG and 16 MG Tablets.: Summary of Product CharacteristicsDokument20 SeitenAtacand 4 MG, 8 MG and 16 MG Tablets.: Summary of Product CharacteristicsasdwasdNoch keine Bewertungen
- Clinical Pharmacy 2023-2024 Lectures - 2Dokument104 SeitenClinical Pharmacy 2023-2024 Lectures - 2ameerjawad150Noch keine Bewertungen
- 5 HypertensionDokument8 Seiten5 Hypertensioniraqeana100100Noch keine Bewertungen
- ACE Inhibitors PrintDokument5 SeitenACE Inhibitors PrintBernard TangNoch keine Bewertungen
- Ace Inhibutors MailDokument5 SeitenAce Inhibutors MailWendy AdaoNoch keine Bewertungen
- Cardiac MedicationsDokument9 SeitenCardiac Medicationsnovikane100% (1)
- Hypertension Lecture3: Pharmacological TreatmentDokument25 SeitenHypertension Lecture3: Pharmacological TreatmentRam NiwasNoch keine Bewertungen
- 2017 Guideline for High Blood Pressure ManagementDokument3 Seiten2017 Guideline for High Blood Pressure ManagementSydrex SarmientoNoch keine Bewertungen
- CarvedilolDokument3 SeitenCarvedilolapi-3797941100% (3)
- Generic Name Captopril Brand NamesDokument18 SeitenGeneric Name Captopril Brand NamesAiko Villacortes100% (1)
- Guideline Directed Medical Therapy in Heart Failure with Reduced Ejection FractionDokument66 SeitenGuideline Directed Medical Therapy in Heart Failure with Reduced Ejection FractionZosmasNoch keine Bewertungen
- Pharmacological-Management-of-HypertensionDokument35 SeitenPharmacological-Management-of-Hypertensiontf.almutairi88Noch keine Bewertungen
- Cardiac DrugsDokument35 SeitenCardiac DrugsCristina Centurion100% (3)
- Hypertension: Silent KillerDokument28 SeitenHypertension: Silent KilleribratiNoch keine Bewertungen
- Stopp Start ToolkitDokument22 SeitenStopp Start ToolkitRifky IlhamiNoch keine Bewertungen
- Resumen The Seventh Report of The JointDokument4 SeitenResumen The Seventh Report of The JointMARIANA GARCIA LOPEZNoch keine Bewertungen
- Effects of An Angiotensin 2 Receptor Blocker Plus Diuretic Combination Drug in Chronic Heart Failure Complicated by HypertensionDokument7 SeitenEffects of An Angiotensin 2 Receptor Blocker Plus Diuretic Combination Drug in Chronic Heart Failure Complicated by HypertensionDhilah Harfadhilah FakhirahNoch keine Bewertungen
- Farmakologi 1 Antihypertension: NURUL HASANAH (1800085)Dokument31 SeitenFarmakologi 1 Antihypertension: NURUL HASANAH (1800085)MutiaraBintangNoch keine Bewertungen
- Acute Decompensated Heart FailureDokument31 SeitenAcute Decompensated Heart Failure568563Noch keine Bewertungen
- CHF 5Dokument2 SeitenCHF 5Agus HaryantoNoch keine Bewertungen
- Antihypertensive Pharmacologic Agents: Nr33 K Burger, Msed, MSN, RN, CneDokument28 SeitenAntihypertensive Pharmacologic Agents: Nr33 K Burger, Msed, MSN, RN, CneLopez JoeNoch keine Bewertungen
- HypertensionDokument10 SeitenHypertensionaa zzNoch keine Bewertungen
- 1210 DIASTOLIC HypertensionDokument44 Seiten1210 DIASTOLIC HypertensionBoysz TheBestNoch keine Bewertungen
- Manage and Treat HypertensionDokument30 SeitenManage and Treat HypertensionAndreea BocicorNoch keine Bewertungen
- Drug StudyDokument3 SeitenDrug Studyanon_11638632Noch keine Bewertungen
- Study Guide For Final Pharmacology HypertensionDokument39 SeitenStudy Guide For Final Pharmacology HypertensionAlejandro Daniel Landa MoralesNoch keine Bewertungen
- Digoxin Drug CardDokument1 SeiteDigoxin Drug CardMahsa Ahmadzadeh100% (2)
- Heart FailureDokument6 SeitenHeart FailureNatasha MarksNoch keine Bewertungen
- Dokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedDokument54 SeitenDokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedMahmoud FathyNoch keine Bewertungen
- Buletin Farmasi 06/2013Dokument12 SeitenBuletin Farmasi 06/2013afiq83Noch keine Bewertungen
- Drugs for Hypertension 2023 (1)Dokument19 SeitenDrugs for Hypertension 2023 (1)aguilarjanicaNoch keine Bewertungen
- AtorvastatinDokument7 SeitenAtorvastatinKrima PatelNoch keine Bewertungen
- Nutrition in Plants and AnimalsDokument3 SeitenNutrition in Plants and AnimalsHaris Ur RehmanNoch keine Bewertungen
- Risk For Decreased Cardiac OutputDokument4 SeitenRisk For Decreased Cardiac Outputapi-283482759Noch keine Bewertungen
- Chapter 3 Science Form 4Dokument30 SeitenChapter 3 Science Form 4Shafie BuyaminNoch keine Bewertungen
- How Sleeping Positions Impact Sleep Quality and HealthDokument2 SeitenHow Sleeping Positions Impact Sleep Quality and HealthNeelesh Suteri0% (1)
- Foot and Ankle ArthrokinematicsDokument6 SeitenFoot and Ankle ArthrokinematicsCraig StewartNoch keine Bewertungen
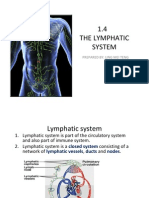
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDokument15 Seiten1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNoch keine Bewertungen
- The Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Dokument5 SeitenThe Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Sinem SerapNoch keine Bewertungen
- Tetanus Neonatorum LectureDokument11 SeitenTetanus Neonatorum LectureJackNoch keine Bewertungen
- 2018 Biology Exercises For SPM (Chapter6 & Chapter7)Dokument15 Seiten2018 Biology Exercises For SPM (Chapter6 & Chapter7)Kuen Jian LinNoch keine Bewertungen
- A Kinesiological Analysis of Shot BY WILLISDokument16 SeitenA Kinesiological Analysis of Shot BY WILLISNoraina AbdullahNoch keine Bewertungen
- L.D..Occlusion in FPDDokument138 SeitenL.D..Occlusion in FPDApurva Deshmukh67% (3)
- Haemoglobin: DR Nilesh Kate MBBS, MD Associate ProfDokument31 SeitenHaemoglobin: DR Nilesh Kate MBBS, MD Associate ProfMarcellia100% (1)
- Photosynthesis Question Booklet: Name . .Dokument16 SeitenPhotosynthesis Question Booklet: Name . .ajithaNoch keine Bewertungen
- 8Dokument6 Seiten8rajanNoch keine Bewertungen
- Biochem QbankDokument16 SeitenBiochem Qbank786waqar786Noch keine Bewertungen
- Head to Toe Physical Assessment GuideDokument16 SeitenHead to Toe Physical Assessment Guideabagatsing100% (5)
- Cell Cycle Lesson PlanDokument4 SeitenCell Cycle Lesson PlanJustine Pama94% (17)
- CHAPTER SUMMARY-opiod AnalgesicDokument9 SeitenCHAPTER SUMMARY-opiod AnalgesicNuttiya WerawattanachaiNoch keine Bewertungen
- Anatomy of A ClamDokument6 SeitenAnatomy of A ClamRU VickNoch keine Bewertungen
- Anesthesia For The Pet Practitioner (2011 3rd Edition)Dokument216 SeitenAnesthesia For The Pet Practitioner (2011 3rd Edition)Amela Dolittle Halilbašić100% (5)
- BTLDokument60 SeitenBTLCamiNoch keine Bewertungen
- Hematology Analyzers, Coagulation Systems Product GuideDokument4 SeitenHematology Analyzers, Coagulation Systems Product GuideElvan Dwi WidyadiNoch keine Bewertungen
- Personal IdentificationDokument13 SeitenPersonal IdentificationJose Li ToNoch keine Bewertungen
- Biology PDFDokument1.447 SeitenBiology PDFPrincess Ethel Atillo100% (2)
- Mechanisms of Cardiac Arrhythmias From Automatici+Dokument24 SeitenMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanNoch keine Bewertungen
- Refeeding SyndromeDokument4 SeitenRefeeding SyndromeallyNoch keine Bewertungen
- SGD Physiology Endocrine and MetabolismDokument7 SeitenSGD Physiology Endocrine and MetabolismTinesh RajahNoch keine Bewertungen
- Modul Anatomi Blok 7Dokument27 SeitenModul Anatomi Blok 7Dewandaru I A BNoch keine Bewertungen
- 1-Aarogyam 1.2 - PO4080828012-204Dokument10 Seiten1-Aarogyam 1.2 - PO4080828012-204jannyyatinNoch keine Bewertungen
- Template POMRDokument8 SeitenTemplate POMRPPDS IPD ULMNoch keine Bewertungen