Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- QBA Award Nomination for Macao Ferry TerminalDokument6 SeitenQBA Award Nomination for Macao Ferry TerminalrishiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shayan - Leading Project Implementation - AmendmentsDokument23 SeitenShayan - Leading Project Implementation - AmendmentsrishiNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- M6.06 - Leading Project ImplementationDokument4 SeitenM6.06 - Leading Project ImplementationrishiNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Mark Sheet: Work Based Assignment M6.06: Leading Project ImplementationDokument2 SeitenMark Sheet: Work Based Assignment M6.06: Leading Project ImplementationrishiNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Articulated WallingDokument24 SeitenArticulated WallingYT LokeNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Tool Durability Proc RoySocDokument21 SeitenTool Durability Proc RoySocrishiNoch keine Bewertungen
- Gsa Usc Shell OfficeDokument36 SeitenGsa Usc Shell OfficeIPutu Reynaldy AryawijayaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Structural Reliability Handbook 2015 PDFDokument47 SeitenStructural Reliability Handbook 2015 PDFrishiNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Real-Time Heat Input Monitoring Towards Robust GMA Brazing: Science and Technology of Welding and JoiningDokument12 SeitenReal-Time Heat Input Monitoring Towards Robust GMA Brazing: Science and Technology of Welding and JoiningrishiNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Assessment Task 1Dokument15 SeitenAssessment Task 1rishiNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Residential Footing DesignDokument26 SeitenResidential Footing Designrishi100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Important AssignmentDokument18 SeitenImportant AssignmentrishiNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 10 1016@j Jclepro 2019 06 032Dokument56 Seiten10 1016@j Jclepro 2019 06 032rishiNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Mobile Comm. PrinciplesDokument23 SeitenMobile Comm. Principlesn2hj2nNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Role of Social Media Marketing On Brand Equity-A Literature ReviewDokument10 SeitenThe Role of Social Media Marketing On Brand Equity-A Literature ReviewrishiNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Role of Social Media Marketing On Brand Equity-A Literature ReviewDokument10 SeitenThe Role of Social Media Marketing On Brand Equity-A Literature ReviewrishiNoch keine Bewertungen
- Question 2Dokument3 SeitenQuestion 2rishiNoch keine Bewertungen
- Force Field AnalysisDokument4 SeitenForce Field AnalysisrishiNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- LAw AssignmentDokument15 SeitenLAw AssignmentrishiNoch keine Bewertungen
- Sample ProposalDokument39 SeitenSample ProposalrishiNoch keine Bewertungen
- Group 4 - Hasbro and MattelDokument15 SeitenGroup 4 - Hasbro and MattelrishiNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Impact of Leadership Styles On Business Success A Case Study On Smes Inamman 2223 5833 1000343Dokument9 SeitenThe Impact of Leadership Styles On Business Success A Case Study On Smes Inamman 2223 5833 1000343rishiNoch keine Bewertungen
- Social Support, Stress, and AdaptationDokument9 SeitenSocial Support, Stress, and AdaptationFarhan SarwarNoch keine Bewertungen
- Comprehensive Research Proposal Example 1Dokument68 SeitenComprehensive Research Proposal Example 1orakzai_496_54783150100% (2)
- Effects of Business Cultural EnvironmentsDokument15 SeitenEffects of Business Cultural EnvironmentsrishiNoch keine Bewertungen
- Critical Evaluation of The Influence of Social Media in The Field of AdvertisingDokument28 SeitenCritical Evaluation of The Influence of Social Media in The Field of AdvertisingrishiNoch keine Bewertungen
- Strengths and Limitations of The Research DesignsDokument9 SeitenStrengths and Limitations of The Research DesignsrishiNoch keine Bewertungen
- Assignment 2Dokument8 SeitenAssignment 2rishiNoch keine Bewertungen
- Self-Awareness as a Therapeutic Tool for Nurse/Client RelationshipDokument6 SeitenSelf-Awareness as a Therapeutic Tool for Nurse/Client RelationshiprishiNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- PrefaceDokument16 SeitenPrefaceNavaneeth RameshNoch keine Bewertungen
- M88A2 Recovery VehicleDokument2 SeitenM88A2 Recovery VehicleJuan CNoch keine Bewertungen
- Christmasworld Trend Brochure 2024Dokument23 SeitenChristmasworld Trend Brochure 2024Ольга ffNoch keine Bewertungen
- 7 - Lakhs Bank EstimateDokument8 Seiten7 - Lakhs Bank Estimatevikram Bargur67% (3)
- OrcaSecurity Solution OverviewDokument2 SeitenOrcaSecurity Solution Overviewandini eldanantyNoch keine Bewertungen
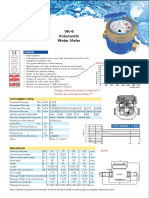
- Baylan: VK-6 Volumetric Water MeterDokument1 SeiteBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaNoch keine Bewertungen
- Secure Access Control and Browser Isolation PrinciplesDokument32 SeitenSecure Access Control and Browser Isolation PrinciplesSushant Yadav100% (1)
- E4PA OmronDokument8 SeitenE4PA OmronCong NguyenNoch keine Bewertungen
- GeM Bidding 2568310Dokument9 SeitenGeM Bidding 2568310SICURO INDIANoch keine Bewertungen
- Manual Centrifugadora - Jouan B4i - 2Dokument6 SeitenManual Centrifugadora - Jouan B4i - 2Rita RosadoNoch keine Bewertungen
- Loans and AdvanceDokument8 SeitenLoans and AdvanceDjay SlyNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 110 TOP Single Phase Induction Motors - Electrical Engineering Multiple Choice Questions and Answers - MCQs Preparation For Engineering Competitive ExamsDokument42 Seiten110 TOP Single Phase Induction Motors - Electrical Engineering Multiple Choice Questions and Answers - MCQs Preparation For Engineering Competitive Examsvijay_marathe01Noch keine Bewertungen
- TMA - ExerciseDokument3 SeitenTMA - ExercisemorrisioNoch keine Bewertungen
- Grid Xtreme VR Data Sheet enDokument3 SeitenGrid Xtreme VR Data Sheet enlong bạchNoch keine Bewertungen
- WebquestDokument3 SeitenWebquestapi-501133650Noch keine Bewertungen
- Online and Payment SecurityDokument14 SeitenOnline and Payment SecurityVanezz UchihaNoch keine Bewertungen
- An-7004 IGBT Driver Calculation Rev00Dokument8 SeitenAn-7004 IGBT Driver Calculation Rev00Raghuram YaramatiNoch keine Bewertungen
- Operations Management For Competitive Advantage 11Th Edition Solutions Manual PDFDokument2 SeitenOperations Management For Competitive Advantage 11Th Edition Solutions Manual PDFLouis DodsonNoch keine Bewertungen
- Salesforce Platform Developer 1Dokument15 SeitenSalesforce Platform Developer 1Kosmic PowerNoch keine Bewertungen
- CP Exit Srategy Plan TemplateDokument4 SeitenCP Exit Srategy Plan TemplateKristia Stephanie BejeranoNoch keine Bewertungen
- Kooltherm PipeDokument8 SeitenKooltherm Pipenaseema1Noch keine Bewertungen
- What Is PID - TutorialDokument5 SeitenWhat Is PID - Tutorialsocrates19582405Noch keine Bewertungen
- Jurisdiction of The Supreme CourtDokument1 SeiteJurisdiction of The Supreme CourtAnshul Yadav100% (1)
- QA InspectionDokument4 SeitenQA Inspectionapi-77180770Noch keine Bewertungen
- Eileen MarcelDokument3 SeitenEileen Marcelapi-3825833Noch keine Bewertungen
- Whitmore EZ-Switch LubricantDokument1 SeiteWhitmore EZ-Switch LubricantDon HowardNoch keine Bewertungen
- Gilette Case - V3Dokument23 SeitenGilette Case - V3Vidar Halvorsen100% (3)
- Memo in Motion For ContemptDokument118 SeitenMemo in Motion For ContemptMark SternNoch keine Bewertungen
- Ceoeg-Cebqn Rev0Dokument3 SeitenCeoeg-Cebqn Rev0jbarbosaNoch keine Bewertungen
- Business Law and The Regulation of Business 12th Edition Mann Test BankDokument25 SeitenBusiness Law and The Regulation of Business 12th Edition Mann Test BankElizabethRuizrxka100% (60)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Epic Measures: One Doctor. Seven Billion Patients.Von EverandEpic Measures: One Doctor. Seven Billion Patients.Bewertung: 4 von 5 Sternen4/5 (13)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineVon EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNoch keine Bewertungen
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsVon EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsBewertung: 4.5 von 5 Sternen4.5/5 (5)
- The Nocebo Effect: When Words Make You SickVon EverandThe Nocebo Effect: When Words Make You SickNoch keine Bewertungen
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusVon EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusBewertung: 4.5 von 5 Sternen4.5/5 (10)