Das könnte Ihnen auch gefallen
- PT Management of Spinal Cord InjuryDokument20 SeitenPT Management of Spinal Cord InjuryJen Passilan100% (1)
- Recent Advances in PhysiotherapyVon EverandRecent Advances in PhysiotherapyCecily PartridgeNoch keine Bewertungen
- Guide To PT PracticeDokument98 SeitenGuide To PT PracticeKana AmesNoch keine Bewertungen
- Cervical Assessment Form 2014Dokument2 SeitenCervical Assessment Form 2014Mark Koval100% (1)
- Shoulder Disorders, A Simple Guide To The condition, Diagnosis, Treatment And Improvised TreatmentVon EverandShoulder Disorders, A Simple Guide To The condition, Diagnosis, Treatment And Improvised TreatmentBewertung: 5 von 5 Sternen5/5 (1)
- Traumatic Brain Injury Physiotherapy AssessmentDokument20 SeitenTraumatic Brain Injury Physiotherapy AssessmentNithin Nair100% (1)
- Spinal Cord InjuryDokument37 SeitenSpinal Cord InjuryMrmonstrosityNoch keine Bewertungen
- Adhesive Capsulitis, (Frozen Shoulder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandAdhesive Capsulitis, (Frozen Shoulder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Intoduction To MaitlandDokument25 SeitenIntoduction To MaitlandAsad Chaudhary100% (1)
- Physiotherapy in Alopecia AreataDokument21 SeitenPhysiotherapy in Alopecia AreataAngel100% (2)
- Books PhysiotherapyDokument22 SeitenBooks Physiotherapyroyalviren100% (2)
- The Role of Physiotherapy in RehabilitationDokument5 SeitenThe Role of Physiotherapy in Rehabilitationari_alianiNoch keine Bewertungen
- Diabetes and PhysiotherapyDokument15 SeitenDiabetes and Physiotherapyane2saNoch keine Bewertungen
- Physiotherapy Management of Tennis Elbow................ ArticleDokument5 SeitenPhysiotherapy Management of Tennis Elbow................ ArticleRupika SodhiNoch keine Bewertungen
- Physiotherapy in General Surgical ConditionDokument7 SeitenPhysiotherapy in General Surgical Conditionprofpt98100% (8)
- 2 Year Physical Therapy NotesDokument129 Seiten2 Year Physical Therapy Notesthwiseman94% (17)
- MPT Books ListDokument3 SeitenMPT Books ListImran KhanNoch keine Bewertungen
- Physical Therapy Board Review 1e by Brad Fortinberry PT DPT Scs Michael Dunaway PT 1560534974Dokument5 SeitenPhysical Therapy Board Review 1e by Brad Fortinberry PT DPT Scs Michael Dunaway PT 1560534974Ivan CasaresNoch keine Bewertungen
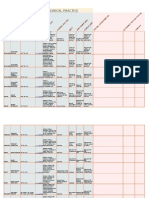
- Specialist Physiotherapy Assessment FormDokument4 SeitenSpecialist Physiotherapy Assessment FormSathish Kumar100% (2)
- Ethics in Physical Therapy PracticeDokument41 SeitenEthics in Physical Therapy PracticemilananandNoch keine Bewertungen
- Cardio Pulmonary AssessmentDokument7 SeitenCardio Pulmonary AssessmentRaj KannanNoch keine Bewertungen
- Manual Therapy Assessment FormDokument8 SeitenManual Therapy Assessment FormPraveenkumar CrNoch keine Bewertungen
- Role of Physiotherapy in Management of Burns-HshDokument25 SeitenRole of Physiotherapy in Management of Burns-HshChristopher Chibueze Igbo100% (1)
- The Indian Association of Physiotherapists - IAP Constitutions PDFDokument17 SeitenThe Indian Association of Physiotherapists - IAP Constitutions PDFHasan RahmanNoch keine Bewertungen
- Resisted ExerciseDokument29 SeitenResisted ExerciseVaraNoch keine Bewertungen
- Ebook PTDokument24 SeitenEbook PTMuhammad NurtiyantoNoch keine Bewertungen
- Physiotherapy ManagementDokument137 SeitenPhysiotherapy ManagementLavanya AuthimooalmNoch keine Bewertungen
- Physiotherapy Assessment For Orthopedic ConditionsDokument6 SeitenPhysiotherapy Assessment For Orthopedic ConditionsSHAIK SHABEENA100% (3)
- Musculoskeletal - Physiotherapy - Amy WashbrookDokument35 SeitenMusculoskeletal - Physiotherapy - Amy WashbrookRaluca Andreea100% (1)
- Cardio Alexandra Hough 2nd EditionDokument376 SeitenCardio Alexandra Hough 2nd EditionManoj M100% (1)
- Supraspinatus TendinitisDokument7 SeitenSupraspinatus Tendinitismilananand100% (1)
- Sports Medicine Specialists Rehabilitation ProtocolsDokument59 SeitenSports Medicine Specialists Rehabilitation ProtocolsThe Homie100% (2)
- Orthopedic Physiotherapy AssessmentDokument2 SeitenOrthopedic Physiotherapy AssessmentVijaya KrishnaNoch keine Bewertungen
- Interferential TherapyDokument31 SeitenInterferential TherapyFaisal Qureshi89% (9)
- Cyriax IntroDokument14 SeitenCyriax IntrodrrajmptnNoch keine Bewertungen
- PNF BasicsDokument38 SeitenPNF Basicsbpt2100% (3)
- Guidelines To Physical Therapist Practice APTADokument1.006 SeitenGuidelines To Physical Therapist Practice APTAGustavo Cabanas82% (11)
- General Physiotherapy AssessmentDokument2 SeitenGeneral Physiotherapy AssessmentRajeev Tiwari75% (4)
- A Guide To Physical Therapist Practice. Volume I PDFDokument58 SeitenA Guide To Physical Therapist Practice. Volume I PDFRamiro Tabilo Maluenda100% (1)
- Cervical SpineDokument177 SeitenCervical SpineJayaRakMinimarketNoch keine Bewertungen
- Soft Tissue InjuriesDokument14 SeitenSoft Tissue Injurieskrissh20100% (2)
- Spinal Cord Injury Physical Therapy ManagementDokument86 SeitenSpinal Cord Injury Physical Therapy ManagementSmithesh OkNoch keine Bewertungen
- Pulmonary Physical Therapy RevDokument11 SeitenPulmonary Physical Therapy Revpearl042008100% (2)
- Physiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeDokument9 SeitenPhysiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeHumaira RahmanNoch keine Bewertungen
- Physical Therapy Evaluation FormDokument2 SeitenPhysical Therapy Evaluation Formapi-400891334Noch keine Bewertungen
- DR Vaishali - Therapeutic GymnasiumDokument35 SeitenDR Vaishali - Therapeutic Gymnasiumvaishali jagtapNoch keine Bewertungen
- Physiotherapy in Pediatrics - NEURO MUSCULAR CONDITIONSDokument28 SeitenPhysiotherapy in Pediatrics - NEURO MUSCULAR CONDITIONSKumar G PalaniNoch keine Bewertungen
- Physiotherapy For Osteoarthritis of The Knee PDFDokument391 SeitenPhysiotherapy For Osteoarthritis of The Knee PDFPipi KNoch keine Bewertungen
- The Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityDokument6 SeitenThe Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityInternational Journal of Physiotherapy and ResearchNoch keine Bewertungen
- Manual Therapy TechniquesDokument30 SeitenManual Therapy TechniquesNistara Singh Chawla100% (1)
- Physical Agent ModalitiesDokument8 SeitenPhysical Agent ModalitiesTrisha Regalado100% (1)
- Therapeutic Exercise Foundation ConceptsDokument13 SeitenTherapeutic Exercise Foundation ConceptsAngelic khanNoch keine Bewertungen
- Upper Limb Fractures - Physiotherapy PDFDokument52 SeitenUpper Limb Fractures - Physiotherapy PDFaliprasanna85% (13)
- Physiotherapy Care Protocol For Shoulder Pain Update MayDokument55 SeitenPhysiotherapy Care Protocol For Shoulder Pain Update May28111966100% (2)
- Biomechanics of SpineDokument22 SeitenBiomechanics of Spineyuvraj100% (1)
- Mastectomy and Physiotherapy Management Final YearDokument24 SeitenMastectomy and Physiotherapy Management Final YearNithin Nair57% (7)
- Orthopedic Assessment For PhysiotherapistDokument3 SeitenOrthopedic Assessment For Physiotherapistsenthilkumar76% (21)
- Basic Neurophysiologic Principles For PNFDokument5 SeitenBasic Neurophysiologic Principles For PNFdramitsainiNoch keine Bewertungen
- 05 - Elderly Falls Test ProcedureDokument1 Seite05 - Elderly Falls Test ProceduredramitsainiNoch keine Bewertungen
- Goniometry For Clinical PracticeDokument7 SeitenGoniometry For Clinical Practicedramitsaini33% (3)
- List of Banned MedicineDokument2 SeitenList of Banned MedicinedramitsainiNoch keine Bewertungen
- (Handbook of Exploration Geochemistry 5) KALEVI KAURANNE (Eds.) - Regolith Exploration Geochemistry in Arctic and Temperate Terrains-Elsevier Science (1992) PDFDokument445 Seiten(Handbook of Exploration Geochemistry 5) KALEVI KAURANNE (Eds.) - Regolith Exploration Geochemistry in Arctic and Temperate Terrains-Elsevier Science (1992) PDFSam BasNoch keine Bewertungen
- Gelernter, David Hillel - The Tides of Mind - Uncovering The Spectrum of Consciousness-Liveright Publishing Corporation (2016)Dokument263 SeitenGelernter, David Hillel - The Tides of Mind - Uncovering The Spectrum of Consciousness-Liveright Publishing Corporation (2016)রশুদ্দি হাওলাদার100% (2)
- Project ExtensionDokument27 SeitenProject Extensionrajith rajeevNoch keine Bewertungen
- Behind The Scrubs: Monica Velarde Saint Mary's College December 09, 2008Dokument21 SeitenBehind The Scrubs: Monica Velarde Saint Mary's College December 09, 2008EthanNoch keine Bewertungen
- Pain Assessment AND Management: Mr. Swapnil Wanjari Clinical InstructorDokument27 SeitenPain Assessment AND Management: Mr. Swapnil Wanjari Clinical InstructorSWAPNIL WANJARINoch keine Bewertungen
- NLS Arabic and French Issue R12.1.3Dokument7 SeitenNLS Arabic and French Issue R12.1.3Anil RawatNoch keine Bewertungen
- Kenoyer, Jonathan M. & Heather ML Miller, Metal technologies of the Indus valley tradition in Pakistan and Western India, in: The Archaeometallurgy of the Asian Old World, 1999, ed. by VC Piggott, Philadelphia, Univ. of Pennsylvania Museum, pp.107-151Dokument46 SeitenKenoyer, Jonathan M. & Heather ML Miller, Metal technologies of the Indus valley tradition in Pakistan and Western India, in: The Archaeometallurgy of the Asian Old World, 1999, ed. by VC Piggott, Philadelphia, Univ. of Pennsylvania Museum, pp.107-151Srini KalyanaramanNoch keine Bewertungen
- Prompts QueryDokument4 SeitenPrompts Querysatyanarayana NVSNoch keine Bewertungen
- Readable Elaine Kirn - Pamela Hartmenn, - 2009 - Interactions 1 - EnG 106 - 2020S - TEXTDokument256 SeitenReadable Elaine Kirn - Pamela Hartmenn, - 2009 - Interactions 1 - EnG 106 - 2020S - TEXTle huy100% (1)
- Stetment 10 PDFDokument4 SeitenStetment 10 PDFvaraprasadNoch keine Bewertungen
- 1st-Year ObliconDokument10 Seiten1st-Year ObliconIts SaoirseNoch keine Bewertungen
- Katehi Grievance LetterDokument12 SeitenKatehi Grievance LetterSacramento BeeNoch keine Bewertungen
- 3 C FamilyIImoot2015Dokument3 Seiten3 C FamilyIImoot2015ApoorvaChandraNoch keine Bewertungen
- Intussusception in Children - UpToDate PDFDokument38 SeitenIntussusception in Children - UpToDate PDFwisdom loverNoch keine Bewertungen
- Aja052550590 786Dokument13 SeitenAja052550590 786EugeneSeasoleNoch keine Bewertungen
- 50 BridgesDokument79 Seiten50 BridgesTeo Wei KeongNoch keine Bewertungen
- Zambian Open University: School of Social Science and HumanitiesDokument9 SeitenZambian Open University: School of Social Science and HumanitiesEvangelist Kabaso SydneyNoch keine Bewertungen
- OODBSDokument29 SeitenOODBSMinh Tu TranNoch keine Bewertungen
- Alphabet Series Tricks - PDF: Down During Your ExamDokument8 SeitenAlphabet Series Tricks - PDF: Down During Your ExamJoshNoch keine Bewertungen
- FACIAL NERVE ParalysisDokument35 SeitenFACIAL NERVE ParalysisIgnasNoch keine Bewertungen
- The Essence of Man enDokument170 SeitenThe Essence of Man enralforoniNoch keine Bewertungen
- Choral Speaking - Our School LifeDokument4 SeitenChoral Speaking - Our School LifeAINA AZMINA BINTI ANUAR KPM-GuruNoch keine Bewertungen
- DP Biology - Speciation Lesson PlanDokument2 SeitenDP Biology - Speciation Lesson Planapi-257190713100% (1)
- Orgl 4361 Capstone 2 Artifact ResearchDokument12 SeitenOrgl 4361 Capstone 2 Artifact Researchapi-531401638Noch keine Bewertungen
- The Intentionality of Sensation A Grammatical Feature GEM Anscombe PDFDokument21 SeitenThe Intentionality of Sensation A Grammatical Feature GEM Anscombe PDFLorenz49Noch keine Bewertungen
- A Written Report in Pure Monopoly: Submitted ToDokument12 SeitenA Written Report in Pure Monopoly: Submitted ToEd Leen ÜNoch keine Bewertungen
- Appeal For Exclusion COA For An Act Committed in Good FaithDokument13 SeitenAppeal For Exclusion COA For An Act Committed in Good FaithPj Tigniman100% (6)
- Additional Mathematics Project Work Kelantan 2/2012Dokument29 SeitenAdditional Mathematics Project Work Kelantan 2/2012Muhammad Afif44% (9)
- Quantitative Option Strategies: Marco Avellaneda G63.2936.001 Spring Semester 2009Dokument29 SeitenQuantitative Option Strategies: Marco Avellaneda G63.2936.001 Spring Semester 2009Adi MNoch keine Bewertungen
- DCF Calculation of Dabur India Ltd.Dokument6 SeitenDCF Calculation of Dabur India Ltd.Radhika ChaudhryNoch keine Bewertungen
- Digital Filmmaking: The Ultimate Guide to Web Video Production for Beginners and Non-Professionals, Learn Useful Tips and Advice on How You Can Create, Film and Edit Your VideosVon EverandDigital Filmmaking: The Ultimate Guide to Web Video Production for Beginners and Non-Professionals, Learn Useful Tips and Advice on How You Can Create, Film and Edit Your VideosBewertung: 5 von 5 Sternen5/5 (1)
- Retro Gaming with Raspberry Pi: Nearly 200 Pages of Video Game ProjectsVon EverandRetro Gaming with Raspberry Pi: Nearly 200 Pages of Video Game ProjectsNoch keine Bewertungen
- The Innovators: How a Group of Hackers, Geniuses, and Geeks Created the Digital RevolutionVon EverandThe Innovators: How a Group of Hackers, Geniuses, and Geeks Created the Digital RevolutionBewertung: 4.5 von 5 Sternen4.5/5 (543)
- INCOSE Systems Engineering Handbook: A Guide for System Life Cycle Processes and ActivitiesVon EverandINCOSE Systems Engineering Handbook: A Guide for System Life Cycle Processes and ActivitiesBewertung: 5 von 5 Sternen5/5 (1)
- Conquering the Electron: The Geniuses, Visionaries, Egomaniacs, and Scoundrels Who Built Our Electronic AgeVon EverandConquering the Electron: The Geniuses, Visionaries, Egomaniacs, and Scoundrels Who Built Our Electronic AgeBewertung: 4.5 von 5 Sternen4.5/5 (10)
- Electrical Engineering 101: Everything You Should Have Learned in School...but Probably Didn'tVon EverandElectrical Engineering 101: Everything You Should Have Learned in School...but Probably Didn'tBewertung: 4.5 von 5 Sternen4.5/5 (27)
- Practical Electrical Wiring: Residential, Farm, Commercial, and IndustrialVon EverandPractical Electrical Wiring: Residential, Farm, Commercial, and IndustrialBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Electronics All-in-One For Dummies, 3rd EditionVon EverandElectronics All-in-One For Dummies, 3rd EditionBewertung: 5 von 5 Sternen5/5 (2)
- Analog Design and Simulation Using OrCAD Capture and PSpiceVon EverandAnalog Design and Simulation Using OrCAD Capture and PSpiceNoch keine Bewertungen
- 2022 Adobe® Premiere Pro Guide For Filmmakers and YouTubersVon Everand2022 Adobe® Premiere Pro Guide For Filmmakers and YouTubersBewertung: 5 von 5 Sternen5/5 (1)
- A Mind at Play: How Claude Shannon Invented the Information AgeVon EverandA Mind at Play: How Claude Shannon Invented the Information AgeBewertung: 4 von 5 Sternen4/5 (53)
- Programming the Raspberry Pi, Third Edition: Getting Started with PythonVon EverandProgramming the Raspberry Pi, Third Edition: Getting Started with PythonBewertung: 5 von 5 Sternen5/5 (2)
- Heat Transfer Engineering: Fundamentals and TechniquesVon EverandHeat Transfer Engineering: Fundamentals and TechniquesBewertung: 4 von 5 Sternen4/5 (1)
- Build Your Own Electronics WorkshopVon EverandBuild Your Own Electronics WorkshopBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Hacking Electronics: An Illustrated DIY Guide for Makers and HobbyistsVon EverandHacking Electronics: An Illustrated DIY Guide for Makers and HobbyistsBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Current Interruption Transients CalculationVon EverandCurrent Interruption Transients CalculationBewertung: 4 von 5 Sternen4/5 (1)
- Practical Power Distribution for IndustryVon EverandPractical Power Distribution for IndustryBewertung: 2.5 von 5 Sternen2.5/5 (2)
- Beginner's Guide to Reading Schematics, Third EditionVon EverandBeginner's Guide to Reading Schematics, Third EditionNoch keine Bewertungen
- Teach Yourself Electricity and Electronics, 6th EditionVon EverandTeach Yourself Electricity and Electronics, 6th EditionBewertung: 3.5 von 5 Sternen3.5/5 (15)