Das könnte Ihnen auch gefallen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument2 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- Booking Confirmation For Process Number 123782146Dokument2 SeitenBooking Confirmation For Process Number 123782146Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument3 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument3 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- HDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Dokument2 SeitenHDFC ERGO General Insurance Company Limited: Policy No. 2320 1001 7259 2300 000Jason RogersNoch keine Bewertungen
- Client Information - ZF INDIA PRIVATE LIMITED: Booking ConfirmationDokument2 SeitenClient Information - ZF INDIA PRIVATE LIMITED: Booking ConfirmationJason RogersNoch keine Bewertungen
- Bank ChequeDokument1 SeiteBank ChequeJason RogersNoch keine Bewertungen
- Receipt 9862882Dokument1 SeiteReceipt 9862882Jason RogersNoch keine Bewertungen
- Letter 1Dokument1 SeiteLetter 1Jason RogersNoch keine Bewertungen
- Powder CoatingDokument36 SeitenPowder CoatingJason Rogers100% (1)
- HYD JD Lead Vehicle DesignerDokument2 SeitenHYD JD Lead Vehicle DesignerJason RogersNoch keine Bewertungen
- Sae J449a 1963Dokument4 SeitenSae J449a 1963Jason RogersNoch keine Bewertungen
- Mohammad Mohiuddin: What'S The Balance On My Card?Dokument3 SeitenMohammad Mohiuddin: What'S The Balance On My Card?Jason RogersNoch keine Bewertungen
- Itp Piping PDFDokument4 SeitenItp Piping PDFdashNoch keine Bewertungen
- Sae J287 1988 PDFDokument50 SeitenSae J287 1988 PDFJason Rogers100% (2)
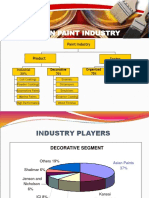
- Market Study of Paint IndustryDokument9 SeitenMarket Study of Paint IndustryJason RogersNoch keine Bewertungen
- Automotive Paint Michael OlveraDokument7 SeitenAutomotive Paint Michael OlveraJason RogersNoch keine Bewertungen
- Parallel ArchitecturesDokument56 SeitenParallel ArchitectureskalscribNoch keine Bewertungen
- Clip Tower Cut OutsDokument1 SeiteClip Tower Cut OutsJason RogersNoch keine Bewertungen
- Tool TestDokument2 SeitenTool TestJason RogersNoch keine Bewertungen
- By Authority of Legally Binding Document: The United States of AmericaDokument10 SeitenBy Authority of Legally Binding Document: The United States of AmericaJason RogersNoch keine Bewertungen
- Sae J902a 1967Dokument5 SeitenSae J902a 1967Jason RogersNoch keine Bewertungen
- Application Note: Antenna Fundamentals: DiscussionDokument4 SeitenApplication Note: Antenna Fundamentals: DiscussioncorsairsanNoch keine Bewertungen
- Wajdi A. S. Khamayseh CV: Objectives and Resume SummaryDokument5 SeitenWajdi A. S. Khamayseh CV: Objectives and Resume SummaryJason RogersNoch keine Bewertungen
- Workholding 1 321methodDokument31 SeitenWorkholding 1 321methodJason RogersNoch keine Bewertungen
- Designing Plastic Components - QMRplasticsDokument10 SeitenDesigning Plastic Components - QMRplasticsClara PereiraNoch keine Bewertungen
- Part and Mold Design Guide (2005)Dokument174 SeitenPart and Mold Design Guide (2005)naitikpanchal100% (4)
- Transmission 240509Dokument25 SeitenTransmission 240509Jason RogersNoch keine Bewertungen
- Crash Analysis 240509Dokument39 SeitenCrash Analysis 240509Jason RogersNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Duplo DP - 440 - 430 - 340 - 330 - ServiceDokument311 SeitenDuplo DP - 440 - 430 - 340 - 330 - Servicemrservak50% (2)
- Sharp AR 5316 - 5320 Service ManualDokument19 SeitenSharp AR 5316 - 5320 Service ManualTehran Copy0% (1)
- Brother DCP b7500d DatasheetDokument2 SeitenBrother DCP b7500d DatasheetJignesh KachariyaNoch keine Bewertungen
- Samsung SCX 4300 InstructionDokument97 SeitenSamsung SCX 4300 InstructionRozhin MoftizadehNoch keine Bewertungen
- Photo Paper SizesDokument3 SeitenPhoto Paper SizessassabossNoch keine Bewertungen
- Application of Cubic Spline Interpolation To Fit The Stress-Strain Curve To SAE 1020 SteelDokument3 SeitenApplication of Cubic Spline Interpolation To Fit The Stress-Strain Curve To SAE 1020 SteelIJAERS JOURNALNoch keine Bewertungen
- Plockmatic BK5030 OpMan (EN)Dokument64 SeitenPlockmatic BK5030 OpMan (EN)Gisell ZapataNoch keine Bewertungen
- I R2016 JDokument4 SeitenI R2016 JStariunNoch keine Bewertungen
- Papercraft SoccerDokument6 SeitenPapercraft SoccerDevi NugrahaNoch keine Bewertungen
- KM 2560 3060ensmr2 PDFDokument392 SeitenKM 2560 3060ensmr2 PDFJustino NievesNoch keine Bewertungen
- TA 3051ci 3551ci 4551ci 5551cibul1Dokument32 SeitenTA 3051ci 3551ci 4551ci 5551cibul1stevanreljicNoch keine Bewertungen
- Desktop PC Intel Core I3 Intel® Core™ I3-6100T Processor (3.20 GHZ, 3M Cache)Dokument6 SeitenDesktop PC Intel Core I3 Intel® Core™ I3-6100T Processor (3.20 GHZ, 3M Cache)Muhammad TaufiqNoch keine Bewertungen
- European Comission Visual Identity ManualDokument223 SeitenEuropean Comission Visual Identity ManualAnDy RacerNoch keine Bewertungen
- Attach-3 Functional Design Specification (FDS)Dokument41 SeitenAttach-3 Functional Design Specification (FDS)Anandharaja RajamohanNoch keine Bewertungen
- International Standard Paper SizesDokument27 SeitenInternational Standard Paper SizesShnur4oNoch keine Bewertungen
- ECOSYS P6021cdn ECOSYS P6026cdn: Service ManualDokument214 SeitenECOSYS P6021cdn ECOSYS P6026cdn: Service ManualАлексей КальченкоNoch keine Bewertungen
- Kyocera FS-6950DN Service ManualDokument128 SeitenKyocera FS-6950DN Service ManualMihai Dan Ambrosie100% (1)
- MX-M264-314-354 ServiceDokument258 SeitenMX-M264-314-354 ServiceLee Donnelly100% (2)
- Folding of Drawing Prints: Indian StandardDokument3 SeitenFolding of Drawing Prints: Indian StandardNirav PatelNoch keine Bewertungen
- Lexmark XM1145 XM3150Dokument8 SeitenLexmark XM1145 XM3150Geovanny Gaspar Suar FlorencioNoch keine Bewertungen
- Canon Irc3220n BrochureDokument8 SeitenCanon Irc3220n BrochureTarek MamdouhNoch keine Bewertungen
- 242 Open Office Org Community ForumDokument10 Seiten242 Open Office Org Community ForumTommy GregersenNoch keine Bewertungen
- Canon Ir 2545 Copier PDFDokument2 SeitenCanon Ir 2545 Copier PDFIsaac Musiwa BandaNoch keine Bewertungen
- Sleeping Raccoon: Level 80 Parts Time To Create 15 HourDokument24 SeitenSleeping Raccoon: Level 80 Parts Time To Create 15 HourleidyNoch keine Bewertungen
- Private Limited Phones DataDokument18 SeitenPrivate Limited Phones DataFortune BuildersNoch keine Bewertungen
- ASIC Design of A High Speed Low Power Circuit For Factorial Calculation Using Ancient Vedic MathematicsDokument10 SeitenASIC Design of A High Speed Low Power Circuit For Factorial Calculation Using Ancient Vedic MathematicsNeem PlantNoch keine Bewertungen
- LFG ContentsDokument2 SeitenLFG Contentseemina13Noch keine Bewertungen
- Non Standarad Dowel PinDokument4 SeitenNon Standarad Dowel Pinjaskaran singhNoch keine Bewertungen
- TRef 2Q03Dokument459 SeitenTRef 2Q03asi33eNoch keine Bewertungen
- KompoZer NotesDokument17 SeitenKompoZer NoteshaffizanNoch keine Bewertungen