Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
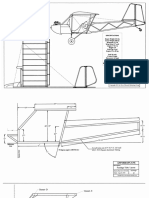
- Plans PDFDokument49 SeitenPlans PDFEstevam Gomes de Azevedo85% (34)
- GCSE AstronomyDokument30 SeitenGCSE Astronomyharris123mc100% (1)
- Soldier of Fortune PDFDokument208 SeitenSoldier of Fortune PDFNixel SpielNoch keine Bewertungen
- Pediatric EmergenciesDokument47 SeitenPediatric EmergenciesahmedNoch keine Bewertungen
- Naming Hydrocarbons Worksheet1 Key 12 26 08 PDFDokument2 SeitenNaming Hydrocarbons Worksheet1 Key 12 26 08 PDFMarilyn Castro Laquindanum100% (1)
- Hydrodynamic Calculation Butterfly Valve (Double Disc)Dokument31 SeitenHydrodynamic Calculation Butterfly Valve (Double Disc)met-calcNoch keine Bewertungen
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDokument5 SeitenAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaNoch keine Bewertungen
- Childhood Urinary Tract Infection in Primary Care:: ResearchDokument7 SeitenChildhood Urinary Tract Infection in Primary Care:: ResearchLavfy NjlaaNoch keine Bewertungen
- Bell 'S Palsy in Children (Bellpic) : Protocol For A Multicentre, Placebo-Controlled Randomized TrialDokument11 SeitenBell 'S Palsy in Children (Bellpic) : Protocol For A Multicentre, Placebo-Controlled Randomized TrialLavfy NjlaaNoch keine Bewertungen
- Jurnal OtitisDokument22 SeitenJurnal OtitisLavfy NjlaaNoch keine Bewertungen
- Lab Report Marketing Mansi 4Dokument39 SeitenLab Report Marketing Mansi 4Mansi SharmaNoch keine Bewertungen
- Paediatric Intake Form Modern OT 2018Dokument6 SeitenPaediatric Intake Form Modern OT 2018SefNoch keine Bewertungen
- Fines Reduction Project at Wendling Bowser QuarryDokument2 SeitenFines Reduction Project at Wendling Bowser QuarryMarcos Antonio ParoliniNoch keine Bewertungen
- LG250CDokument2 SeitenLG250CCarlosNoch keine Bewertungen
- Electricity NotesDokument35 SeitenElectricity Notesapi-277818647Noch keine Bewertungen
- Midterm Exam Gor Grade 11Dokument2 SeitenMidterm Exam Gor Grade 11Algelle AbrantesNoch keine Bewertungen
- Lafarge Interior Building Solutions BrochureDokument24 SeitenLafarge Interior Building Solutions BrochuretwinpixtwinpixNoch keine Bewertungen
- Data Bulletin Group Motor Installations:: Understanding National Electrical Code (NEC) 430.53 RequirementsDokument8 SeitenData Bulletin Group Motor Installations:: Understanding National Electrical Code (NEC) 430.53 RequirementsshoaibNoch keine Bewertungen
- Kinematics in One DimensionDokument4 SeitenKinematics in One DimensionAldrin VillanuevaNoch keine Bewertungen
- Presentation On 4G TechnologyDokument23 SeitenPresentation On 4G TechnologyFresh EpicNoch keine Bewertungen
- SP Essay 1Dokument14 SeitenSP Essay 1api-511870420Noch keine Bewertungen
- GP1 Q1 Week-1Dokument18 SeitenGP1 Q1 Week-1kickyknacksNoch keine Bewertungen
- Main Girders: CrossDokument3 SeitenMain Girders: Crossmn4webNoch keine Bewertungen
- G1CDokument12 SeitenG1CKhriz Ann C ÜNoch keine Bewertungen
- AoS Soulbound - Pregens - Skyrigger Malgra DainssonDokument2 SeitenAoS Soulbound - Pregens - Skyrigger Malgra DainssonAdrien DeschampsNoch keine Bewertungen
- The Light Fantastic by Sarah CombsDokument34 SeitenThe Light Fantastic by Sarah CombsCandlewick PressNoch keine Bewertungen
- Gypsum Plasterboard: National Standard of The People'S Republic of ChinaDokument15 SeitenGypsum Plasterboard: National Standard of The People'S Republic of ChinaGarry100% (2)
- Bulacan Agricultural State College: Lesson Plan in Science 4 Life Cycle of Humans, Animals and PlantsDokument6 SeitenBulacan Agricultural State College: Lesson Plan in Science 4 Life Cycle of Humans, Animals and PlantsHarmonica PellazarNoch keine Bewertungen
- Ali Erdemir: Professional ExperienceDokument3 SeitenAli Erdemir: Professional ExperienceDunkMeNoch keine Bewertungen
- Health Promotion Throughout The Life Span 7th Edition Edelman Test BankDokument35 SeitenHealth Promotion Throughout The Life Span 7th Edition Edelman Test Bankcourtneyharrisbpfyrkateq100% (17)
- Scanner and Xcal Comperative Analysis v2Dokument22 SeitenScanner and Xcal Comperative Analysis v2Ziya2009Noch keine Bewertungen
- Cathodic Protection Catalog - New 8Dokument1 SeiteCathodic Protection Catalog - New 8dhineshNoch keine Bewertungen
- Poly 103Dokument20 SeitenPoly 103Sharifah Zulaikha BenYahyaNoch keine Bewertungen
- Scott 2001Dokument20 SeitenScott 2001Mariana CatiniNoch keine Bewertungen