Das könnte Ihnen auch gefallen
- Test Bank For Microbiology Basic and Clinical Principles 1st Edition Lourdes P Norman MckayDokument8 SeitenTest Bank For Microbiology Basic and Clinical Principles 1st Edition Lourdes P Norman MckayJoseph Williams97% (31)
- United States Patent Application Publication No .: US 2021/0082583 A1Dokument53 SeitenUnited States Patent Application Publication No .: US 2021/0082583 A1Tim Brown100% (7)
- Communicable Diseases ReviewerDokument13 SeitenCommunicable Diseases Reviewerderic88% (17)
- Chapter 24 Prep UDokument9 SeitenChapter 24 Prep UMary Ann CarandangNoch keine Bewertungen
- Hand Hygiene Knowledge Assessment Questionnaire (IHI)Dokument2 SeitenHand Hygiene Knowledge Assessment Questionnaire (IHI)Suseno Aji50% (2)
- Care of Clients With Problems Related To Neurological SystemDokument44 SeitenCare of Clients With Problems Related To Neurological Systemapi-3735995100% (1)
- IV Insertion ProcedureDokument11 SeitenIV Insertion ProcedureEdelweiss Marie Cayetano100% (1)
- Blood Transfusion Nursing Care and AssessmentDokument31 SeitenBlood Transfusion Nursing Care and AssessmentmyNoch keine Bewertungen
- Fall Risk Assessment FormDokument3 SeitenFall Risk Assessment FormMichael Silva100% (1)
- Guidelines in PortfolioDokument3 SeitenGuidelines in PortfolioRaquel M. Mendoza100% (1)
- Pentagon CDDokument12 SeitenPentagon CDJohnNoch keine Bewertungen
- Communicablediseases 110227001506 Phpapp02 PDFDokument30 SeitenCommunicablediseases 110227001506 Phpapp02 PDFCrystal Ann Monsale TadiamonNoch keine Bewertungen
- Completed Concept MapDokument4 SeitenCompleted Concept Mapapi-607361848Noch keine Bewertungen
- Hepatobiliary DisordersDokument2 SeitenHepatobiliary DisordersFreeNursingNotes0% (1)
- STDs Guide: Gonorrhea to SyphilisDokument5 SeitenSTDs Guide: Gonorrhea to Syphilisreghpineda28Noch keine Bewertungen
- Communicable Disease Nursing: An OverviewDokument7 SeitenCommunicable Disease Nursing: An Overviewariane100% (1)
- Grand Coaching: Medical Surgical NursingDokument22 SeitenGrand Coaching: Medical Surgical NursingEsarpy (Nana)Noch keine Bewertungen
- Far Eastern University-Institute of Nursing In-House NursingDokument25 SeitenFar Eastern University-Institute of Nursing In-House Nursingjonasdelacruz1111Noch keine Bewertungen
- Pediatric Vital Sign Normal RangesDokument5 SeitenPediatric Vital Sign Normal Rangestinea nigraNoch keine Bewertungen
- CD 1Dokument13 SeitenCD 1Don MarcusNoch keine Bewertungen
- AUTOIMMUNEDokument75 SeitenAUTOIMMUNEEva Boje-JugadorNoch keine Bewertungen
- Vancomycin Dosing and Monitoring in AdultsDokument1 SeiteVancomycin Dosing and Monitoring in AdultsjulialeoNoch keine Bewertungen
- Anti Neoplastic and Immunosupressant DrugsDokument29 SeitenAnti Neoplastic and Immunosupressant DrugsAshraf Moby100% (1)
- CHNDokument38 SeitenCHNLouie John AbilaNoch keine Bewertungen
- Management of Patients With Neurologic Infections, Autoimmune Disorders & NeuropathiesDokument92 SeitenManagement of Patients With Neurologic Infections, Autoimmune Disorders & NeuropathiesejarnmdNoch keine Bewertungen
- Pharma Gapuz IntroDokument40 SeitenPharma Gapuz IntroHayes CloverNoch keine Bewertungen
- Oxytocin and Methylergonovine Nursing StudyDokument16 SeitenOxytocin and Methylergonovine Nursing StudyDinarkram Rabreca EculNoch keine Bewertungen
- Medicationpart1 110202192115 Phpapp02Dokument10 SeitenMedicationpart1 110202192115 Phpapp02Jessamine Rochelle Reyes Esberto100% (1)
- Fluid and Electrolytes, Burns, G.UDokument56 SeitenFluid and Electrolytes, Burns, G.Uapi-3735995100% (4)
- Fluid and Electrolyte NotesDokument6 SeitenFluid and Electrolyte NotesAshley H Locklear100% (1)
- Maternal and Child Health CareDokument7 SeitenMaternal and Child Health CareNessa Layos MorilloNoch keine Bewertungen
- Bulacan State University College of Nursing Final Exam ReviewDokument7 SeitenBulacan State University College of Nursing Final Exam ReviewDemiar Madlansacay QuintoNoch keine Bewertungen
- Fluid, Electrolyte, and Acid-Base BalanceDokument8 SeitenFluid, Electrolyte, and Acid-Base BalanceJo Marchianne PigarNoch keine Bewertungen
- IVY TECH NURSING LAB INFORMATIONDokument7 SeitenIVY TECH NURSING LAB INFORMATIONSethNoch keine Bewertungen
- Normal Lab Values: Complete Blood Count (CBC)Dokument2 SeitenNormal Lab Values: Complete Blood Count (CBC)nabilaNoch keine Bewertungen
- Proper Excreta Disposal, Food Safety and Environmental HealthDokument15 SeitenProper Excreta Disposal, Food Safety and Environmental HealthEden LacsonNoch keine Bewertungen
- BulletsDokument14 SeitenBulletsstuffednurseNoch keine Bewertungen
- Taking Blood PressureDokument3 SeitenTaking Blood PressureApril Iren Claire BalabalaNoch keine Bewertungen
- Pediatric Nursing (Nomral) : Psychiatric (Sigmund Freud) Nursing Concept Range Extends To The 18 MonthDokument6 SeitenPediatric Nursing (Nomral) : Psychiatric (Sigmund Freud) Nursing Concept Range Extends To The 18 MonthVon R SemillaNoch keine Bewertungen
- Our Lady of Fatima University #1 Esperanza St. Hilltop MansionDokument6 SeitenOur Lady of Fatima University #1 Esperanza St. Hilltop Mansionjames garciaNoch keine Bewertungen
- Or NursingDokument14 SeitenOr NursingDharren Rojan Garvida Agullana100% (1)
- Catheterization CHSDokument3 SeitenCatheterization CHSEnriquez AndreanNoch keine Bewertungen
- Fundamentals of NursingDokument127 SeitenFundamentals of NursingChristian Dominic AguinaldeNoch keine Bewertungen
- Osteoporosis Prevention and Fracture Risk ReductionDokument21 SeitenOsteoporosis Prevention and Fracture Risk ReductionrihamNoch keine Bewertungen
- Fhsis PDFDokument216 SeitenFhsis PDFSherina W. EddingNoch keine Bewertungen
- Community Health Nursing Handout PDFDokument27 SeitenCommunity Health Nursing Handout PDFEarl Cordero100% (1)
- COLORECTAL CANCER: SIGNS, STAGES, RISK FACTORS & TREATMENTDokument31 SeitenCOLORECTAL CANCER: SIGNS, STAGES, RISK FACTORS & TREATMENTIrene RealinoNoch keine Bewertungen
- Quiz answers with feedback on nursing questionsDokument7 SeitenQuiz answers with feedback on nursing questionsArlene FerrerNoch keine Bewertungen
- Nursing Chapter 48 Skin Integrity and Wound Care FlashcardsDokument6 SeitenNursing Chapter 48 Skin Integrity and Wound Care FlashcardsMark M. AlipioNoch keine Bewertungen
- NANDA DX NI, NODokument165 SeitenNANDA DX NI, NOKerry Brown100% (1)
- Pharmacology Section on Antibiotics, Antivirals and AntifungalsDokument5 SeitenPharmacology Section on Antibiotics, Antivirals and AntifungalsPathalee ThalpavilaNoch keine Bewertungen
- Mark Fredderick R. Abejo RN, MAN: Maternal and Child Nursing BulletsDokument9 SeitenMark Fredderick R. Abejo RN, MAN: Maternal and Child Nursing BulletsCrystal Ann Monsale TadiamonNoch keine Bewertungen
- Cancer Types, Causes, Symptoms & TreatmentDokument169 SeitenCancer Types, Causes, Symptoms & TreatmentDardarConstantinoNoch keine Bewertungen
- Nursing Care For The Family in Need of Reproductive Life Planning Nursing Care For The Family in Need of Reproductive Life PlanningDokument31 SeitenNursing Care For The Family in Need of Reproductive Life Planning Nursing Care For The Family in Need of Reproductive Life PlanningBridget Shienne DaculaNoch keine Bewertungen
- Eriksons Developmental StagesDokument1 SeiteEriksons Developmental StagesFilipino Nurses CentralNoch keine Bewertungen
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideVon EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNoch keine Bewertungen
- NURSING CARE OF ADULTS II: Passbooks Study GuideVon EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNoch keine Bewertungen
- Community Focused Nursing: Passbooks Study GuideVon EverandCommunity Focused Nursing: Passbooks Study GuideNoch keine Bewertungen
- Registered Professional Nurse: Passbooks Study GuideVon EverandRegistered Professional Nurse: Passbooks Study GuideNoch keine Bewertungen
- Nursing care process in patients with chronic obstructive pulmonary diseaseVon EverandNursing care process in patients with chronic obstructive pulmonary diseaseNoch keine Bewertungen
- Communicable Diseases ReviewerDokument12 SeitenCommunicable Diseases ReviewerEmy TandinganNoch keine Bewertungen
- Difference Between Adult and Fetal CirculationDokument6 SeitenDifference Between Adult and Fetal CirculationRaquel M. MendozaNoch keine Bewertungen
- 3 Problems With The Passenger and Powers of LaborDokument105 Seiten3 Problems With The Passenger and Powers of LaborRaquel M. MendozaNoch keine Bewertungen
- The Family Nursing Process GuideDokument17 SeitenThe Family Nursing Process GuideRaquel M. MendozaNoch keine Bewertungen
- ExpandedroleofnursesDokument17 SeitenExpandedroleofnursesRaquel M. MendozaNoch keine Bewertungen
- 1 The High Risk MotherDokument161 Seiten1 The High Risk MotherRaquel M. MendozaNoch keine Bewertungen
- Care of The NewbornDokument163 SeitenCare of The NewbornRaquel M. MendozaNoch keine Bewertungen
- Growth and Dev Theories2Dokument34 SeitenGrowth and Dev Theories2Raquel M. MendozaNoch keine Bewertungen
- 6 Infancy Diseases 1Dokument135 Seiten6 Infancy Diseases 1Raquel M. MendozaNoch keine Bewertungen
- Growth and Development of Children in the First YearDokument53 SeitenGrowth and Development of Children in the First YearRaquel M. MendozaNoch keine Bewertungen
- Criteria Grading Scale Completion 5 4 3 2: Total PTS: 20Dokument1 SeiteCriteria Grading Scale Completion 5 4 3 2: Total PTS: 20Raquel M. MendozaNoch keine Bewertungen
- Menstrual CycleDokument5 SeitenMenstrual CycleRaquel M. MendozaNoch keine Bewertungen
- Unit Ii Leadership in Nursing: A. Nurse in The OrganizationDokument25 SeitenUnit Ii Leadership in Nursing: A. Nurse in The OrganizationRaquel M. MendozaNoch keine Bewertungen
- Care of The NewbornDokument163 SeitenCare of The NewbornRaquel M. MendozaNoch keine Bewertungen
- 1 The High Risk MotherDokument161 Seiten1 The High Risk MotherRaquel M. MendozaNoch keine Bewertungen
- Growth and Dev Theories2Dokument34 SeitenGrowth and Dev Theories2Raquel M. MendozaNoch keine Bewertungen
- Case Scenario GRP 3Dokument1 SeiteCase Scenario GRP 3Raquel M. MendozaNoch keine Bewertungen
- Qualities of Health Care ProfessionalsDokument23 SeitenQualities of Health Care ProfessionalsRaquel M. MendozaNoch keine Bewertungen
- Criteria Grading Scale Completion 5 4 3 2: Total PTS: 20Dokument1 SeiteCriteria Grading Scale Completion 5 4 3 2: Total PTS: 20Raquel M. MendozaNoch keine Bewertungen
- Grief, Loss, Death and DyingDokument47 SeitenGrief, Loss, Death and DyingRaquel M. MendozaNoch keine Bewertungen
- Med AcronymsDokument15 SeitenMed AcronymsRaquel M. MendozaNoch keine Bewertungen
- Nursing Responsibilities For Medication AdministrationDokument9 SeitenNursing Responsibilities For Medication AdministrationRaquel M. MendozaNoch keine Bewertungen
- Activity and Exercise PatternDokument20 SeitenActivity and Exercise PatternRaquel M. MendozaNoch keine Bewertungen
- Gordon's Functional Health AssessmentDokument11 SeitenGordon's Functional Health AssessmentRaquel M. Mendoza100% (1)
- Activity and ExerciseDokument36 SeitenActivity and ExerciseRaquel M. MendozaNoch keine Bewertungen
- The Healthcare ProviderDokument14 SeitenThe Healthcare ProviderRaquel M. MendozaNoch keine Bewertungen
- Activity and Exercise PatternDokument20 SeitenActivity and Exercise PatternRaquel M. MendozaNoch keine Bewertungen
- Qualities of A Healthcare ProviderDokument6 SeitenQualities of A Healthcare ProviderRaquel M. Mendoza50% (2)
- Communicable DiseasesDokument14 SeitenCommunicable DiseasesRaquel M. MendozaNoch keine Bewertungen
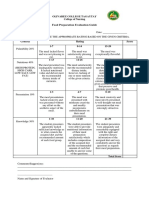
- Food Preparation Evaluation Guide: Olivarez College Tagaytay College of NursingDokument2 SeitenFood Preparation Evaluation Guide: Olivarez College Tagaytay College of NursingRaquel M. MendozaNoch keine Bewertungen
- Antimicrobial effectiveness testingDokument3 SeitenAntimicrobial effectiveness testingKaren Rojas LópezNoch keine Bewertungen
- Format Pendataan Posyandu Sasaran Bian PKM Pondok Gede JatiwaringinDokument407 SeitenFormat Pendataan Posyandu Sasaran Bian PKM Pondok Gede JatiwaringinparamitaNoch keine Bewertungen
- Common Hospital Diseases Requiring Isolation PrecautionsDokument1 SeiteCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNoch keine Bewertungen
- 1,000,000 AND COUNTING: A July Without Roger FedererDokument16 Seiten1,000,000 AND COUNTING: A July Without Roger FedererrtNoch keine Bewertungen
- HFMD: Clinical Features, Complications, Diagnosis and ManagementDokument27 SeitenHFMD: Clinical Features, Complications, Diagnosis and ManagementNur IzzahNoch keine Bewertungen
- Virus or Bacteria - What's The Difference?Dokument1 SeiteVirus or Bacteria - What's The Difference?vallabhaneni rajeshNoch keine Bewertungen
- Parasitology Part 2Dokument124 SeitenParasitology Part 2Mark Angelo JaurigueNoch keine Bewertungen
- Clinical Parasitology Course OverviewDokument58 SeitenClinical Parasitology Course Overview365 DaysNoch keine Bewertungen
- EPI Vaccines: - Inactivated (Killed) Microorganisms - Attentuated Microorganisms Fragments From Microorganisms ToxoidsDokument3 SeitenEPI Vaccines: - Inactivated (Killed) Microorganisms - Attentuated Microorganisms Fragments From Microorganisms ToxoidsIrene Grace BalcuevaNoch keine Bewertungen
- Microbiology Testing and Sterilization Methods for Pharmaceutical ProductsDokument1 SeiteMicrobiology Testing and Sterilization Methods for Pharmaceutical ProductsThomas Niccolo Filamor ReyesNoch keine Bewertungen
- 2.oral Manifestation of Bacterial InfectionDokument18 Seiten2.oral Manifestation of Bacterial Infectionhesti_margarethaNoch keine Bewertungen
- Group A Streptococcus Antibiotic ResistanceDokument8 SeitenGroup A Streptococcus Antibiotic Resistanceselandia nisrinaNoch keine Bewertungen
- Stages of Infection & Chain of InfectionDokument29 SeitenStages of Infection & Chain of Infectionkrenzoolo XDNoch keine Bewertungen
- Bmjopen 2017 July 7 7 Inline Supplementary Material 1 PDFDokument2 SeitenBmjopen 2017 July 7 7 Inline Supplementary Material 1 PDFeyabut1Noch keine Bewertungen
- Silver NanoparticlesDokument12 SeitenSilver NanoparticlesAmina ZoulikhaNoch keine Bewertungen
- DS - Aseptoman® Plus - Pif - en - 1711Dokument2 SeitenDS - Aseptoman® Plus - Pif - en - 1711Serbanica RazvanNoch keine Bewertungen
- Infection and Host ResistanceDokument62 SeitenInfection and Host ResistanceAndrea Marie T. Artajo-BoheromNoch keine Bewertungen
- Full ThesisDokument40 SeitenFull ThesisIskriblihahaNoch keine Bewertungen
- Serious Fungal Infections in The Philippines: Original ArticleDokument5 SeitenSerious Fungal Infections in The Philippines: Original ArticleAilen LagulaNoch keine Bewertungen
- Poxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Dokument10 SeitenPoxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Mestesanu ElisabetaNoch keine Bewertungen
- AMRDokument33 SeitenAMRAbdul TawabNoch keine Bewertungen
- Bloodborne Pathogen Safety TestDokument3 SeitenBloodborne Pathogen Safety TestBlanca AgueroNoch keine Bewertungen
- Kenapa Fungi Ada Kingdom SendiriDokument3 SeitenKenapa Fungi Ada Kingdom SendiriFauzan AzizNoch keine Bewertungen
- Fermented PrelimsDokument11 SeitenFermented PrelimsCarlos Alberto Altamirano CahuancamaNoch keine Bewertungen
- Causative Agents of Yeast InfectionsDokument2 SeitenCausative Agents of Yeast InfectionsDreyden HaloNoch keine Bewertungen
- ReportDokument1 SeiteReportSrinivasateja ReddyNoch keine Bewertungen
- Ow Q 51-100 (14.11.09)Dokument102 SeitenOw Q 51-100 (14.11.09)PradeepNoch keine Bewertungen