Das könnte Ihnen auch gefallen
- Health Advice and Immunizations for TravelersVon EverandHealth Advice and Immunizations for TravelersNoch keine Bewertungen
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Von EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Noch keine Bewertungen
- The Routine Immunisation ScheduleDokument10 SeitenThe Routine Immunisation ScheduleJamesWaitonNoch keine Bewertungen
- Vaccination ScheduleDokument1 SeiteVaccination ScheduleKrishanu BharNoch keine Bewertungen
- EPI Vaccines Revised Oct 2010Dokument18 SeitenEPI Vaccines Revised Oct 2010Jei JayNoch keine Bewertungen
- CHN 2Dokument12 SeitenCHN 2Missy CookNoch keine Bewertungen
- Universal Immnunization ProgramDokument50 SeitenUniversal Immnunization Programnamrata tiwariNoch keine Bewertungen
- Expanded Program On Immunization TrinalDokument2 SeitenExpanded Program On Immunization Trinalagong lodgeNoch keine Bewertungen
- Assignment: Course Packet 04a: Expanded Program On ImmunizationDokument2 SeitenAssignment: Course Packet 04a: Expanded Program On ImmunizationShaira GumaruNoch keine Bewertungen
- Almostadoctor - Co.uk-Vaccination Schedule UKDokument6 SeitenAlmostadoctor - Co.uk-Vaccination Schedule UKIbrahim FoondunNoch keine Bewertungen
- Immunization UipDokument20 SeitenImmunization Uipdevesh gargNoch keine Bewertungen
- Calendario Vacunacion Adultos 2010Dokument4 SeitenCalendario Vacunacion Adultos 2010JOSERUPOLONoch keine Bewertungen
- Immunization AssignmentDokument4 SeitenImmunization Assignmentgadoura95Noch keine Bewertungen
- Children's Medicines: Bell, Edward ADokument16 SeitenChildren's Medicines: Bell, Edward AJonathanNoch keine Bewertungen
- National Immunization ProgramDokument9 SeitenNational Immunization ProgramCriselda PabuaNoch keine Bewertungen
- Immunization - Dr. SarahDokument14 SeitenImmunization - Dr. Sarahf6bk6xnppyNoch keine Bewertungen
- Materi DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformDokument40 SeitenMateri DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformMutiara UtiNoch keine Bewertungen
- Karla May C. Gentapan, M.D. Post-Graduate Medical Intern DMSFI Department of PediatricsDokument66 SeitenKarla May C. Gentapan, M.D. Post-Graduate Medical Intern DMSFI Department of PediatricsCyril James Tagud BualNoch keine Bewertungen
- National Immunization ProgramDokument9 SeitenNational Immunization Programjuanamay30gmailcomNoch keine Bewertungen
- Recommend Ations: S GK, SS, S M, K C, S A, S K D, S V, A KS, S S, S K, H K P, SB, B JP, GVB, P GDokument11 SeitenRecommend Ations: S GK, SS, S M, K C, S A, S K D, S V, A KS, S S, S K, H K P, SB, B JP, GVB, P Ga hNoch keine Bewertungen
- Immunization Division at Mohfw Universal Immunization Program (Uip)Dokument21 SeitenImmunization Division at Mohfw Universal Immunization Program (Uip)Shekhar MishraNoch keine Bewertungen
- SdsadsdadsDokument143 SeitenSdsadsdadsKayeNoch keine Bewertungen
- Immunization StatusDokument21 SeitenImmunization StatusAubery RongNoch keine Bewertungen
- Immuniz Ation: Elaine Frances M. Illo, R.M., R.NDokument50 SeitenImmuniz Ation: Elaine Frances M. Illo, R.M., R.NElaine Frances IlloNoch keine Bewertungen
- Midterm Activity 2 ScitechDokument3 SeitenMidterm Activity 2 ScitechKean KaiNoch keine Bewertungen
- Infant ImmunisationDokument1 SeiteInfant ImmunisationPaul GallagherNoch keine Bewertungen
- Immunization: Expanded Program On Immunization (EPI)Dokument4 SeitenImmunization: Expanded Program On Immunization (EPI)3amabelle arevaloNoch keine Bewertungen
- National Immunization ProgramDokument60 SeitenNational Immunization ProgramPrincess Noreen SavellanoNoch keine Bewertungen
- Vacination NorwayDokument10 SeitenVacination NorwayShankar GunaNoch keine Bewertungen
- Immunization: DR Shahbaz Ahmad Professor Community Medicine Independent Medical College FaisalabadDokument67 SeitenImmunization: DR Shahbaz Ahmad Professor Community Medicine Independent Medical College FaisalabadPriya bhattiNoch keine Bewertungen
- Universal Immunization ProgramDokument15 SeitenUniversal Immunization Programsmruti ranjanNoch keine Bewertungen
- VaccineDokument5 SeitenVaccinekhansa maryamNoch keine Bewertungen
- Vaccines Are For All AgesDokument34 SeitenVaccines Are For All Agesmp1a1234Noch keine Bewertungen
- Introduction To EpiDokument9 SeitenIntroduction To Epihaddi awanNoch keine Bewertungen
- 1 Intro. To Pediatrics &childhood ImmunizationDokument122 Seiten1 Intro. To Pediatrics &childhood ImmunizationOliyad GM AtomsaNoch keine Bewertungen
- Mu 06Dokument5 SeitenMu 06aravindNoch keine Bewertungen
- 0 18yrs ScheduleDokument4 Seiten0 18yrs ScheduleprashantNoch keine Bewertungen
- Vaccines For Your ChildDokument4 SeitenVaccines For Your ChildIftekhar SaikatNoch keine Bewertungen
- 7-18yr Schedule For Immunizations, CDC 2008Dokument1 Seite7-18yr Schedule For Immunizations, CDC 2008Tracy100% (1)
- Iap Vaccination RecentDokument7 SeitenIap Vaccination RecentDrNavya K UmeshNoch keine Bewertungen
- Class IX Science Why Do We Fall Ill PPT Module 3 - 3Dokument17 SeitenClass IX Science Why Do We Fall Ill PPT Module 3 - 3Sandeep Kumar100% (2)
- ImmunizationDokument39 SeitenImmunizationhhh11599Noch keine Bewertungen
- Adult Immunization Schedule by Vaccine and Age Group - CDCDokument17 SeitenAdult Immunization Schedule by Vaccine and Age Group - CDCCamacaro Arevalo JoseNoch keine Bewertungen
- Routine Childhood Immunization Schedule SPRING 2016Dokument1 SeiteRoutine Childhood Immunization Schedule SPRING 2016extraxen3690Noch keine Bewertungen
- Childhood Immunization Lecture For C1Dokument70 SeitenChildhood Immunization Lecture For C1ZmNoch keine Bewertungen
- IMMUNIZATION (Health Education)Dokument33 SeitenIMMUNIZATION (Health Education)Rozel Encarnacion100% (2)
- Vaccine Project - FinalDokument2 SeitenVaccine Project - Finalchelsea garzaNoch keine Bewertungen
- Epi ReviewerDokument4 SeitenEpi ReviewerHannah VueltaNoch keine Bewertungen
- Age of Child Vaccines Needed How and Where It Is GivenDokument1 SeiteAge of Child Vaccines Needed How and Where It Is GivenKwenaNoch keine Bewertungen
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDokument3 SeitenMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
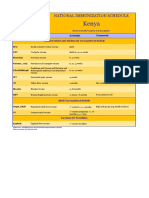
- Kenya Immunization ScheduleDokument1 SeiteKenya Immunization ScheduleDani AnyikaNoch keine Bewertungen
- Mat UkimmunizationDokument4 SeitenMat UkimmunizationNav KovNoch keine Bewertungen
- IMMUNIZATIONDokument35 SeitenIMMUNIZATIONAkshay H.Noch keine Bewertungen
- National Immunization Schedule: For InfantsDokument2 SeitenNational Immunization Schedule: For InfantsRahul DixitNoch keine Bewertungen
- CM - Haem - EPIDokument1 SeiteCM - Haem - EPIRukhsarNoch keine Bewertungen
- VacinationDokument10 SeitenVacinationMostafa Ibrahim AhmedNoch keine Bewertungen
- ImmunizationDokument6 SeitenImmunizationNIKAH PAULINE ALCANTARANoch keine Bewertungen
- EPI Schedule Malawi COM 2017Dokument2 SeitenEPI Schedule Malawi COM 2017INNOCENT KHULIWANoch keine Bewertungen
- Immunization LectureDokument32 SeitenImmunization LectureMekdes ZewdeNoch keine Bewertungen
- Nip Lecture NotesDokument21 SeitenNip Lecture NotesUzziel Galinea TolosaNoch keine Bewertungen
- TetanusDokument2 SeitenTetanusVergaaBellanyNoch keine Bewertungen
- Guideline 7Dokument6 SeitenGuideline 7VergaaBellanyNoch keine Bewertungen
- The Relationship Between Personality Disorders and The Type of CrimeDokument8 SeitenThe Relationship Between Personality Disorders and The Type of CrimeVergaaBellanyNoch keine Bewertungen
- Tetanus PDFDokument11 SeitenTetanus PDFDwi Andriyani NimanNoch keine Bewertungen
- HaemodynamicDokument12 SeitenHaemodynamicVergaaBellanyNoch keine Bewertungen
- Tetanus 20Dokument15 SeitenTetanus 20VergaaBellanyNoch keine Bewertungen
- Guidelines Tetanus 2011Dokument8 SeitenGuidelines Tetanus 2011Nina YuliNoch keine Bewertungen
- 2018 Borderline Personality Symptoms and Work PerformanceDokument9 Seiten2018 Borderline Personality Symptoms and Work PerformanceVergaaBellanyNoch keine Bewertungen
- Neurological Aspects of Tropical Disease-Tetanus8 PDFDokument10 SeitenNeurological Aspects of Tropical Disease-Tetanus8 PDFVergaaBellanyNoch keine Bewertungen
- Tetanus PDFDokument11 SeitenTetanus PDFDwi Andriyani NimanNoch keine Bewertungen
- Relationship Between Borderline Personality Symptoms and Internet Addiction: The Mediating Effects of Mental Health ProblemsDokument8 SeitenRelationship Between Borderline Personality Symptoms and Internet Addiction: The Mediating Effects of Mental Health ProblemsVergaaBellanyNoch keine Bewertungen
- Lest We Forget 18Dokument4 SeitenLest We Forget 18VergaaBellanyNoch keine Bewertungen
- TetanusDokument2 SeitenTetanusVergaaBellanyNoch keine Bewertungen
- mkl014 PDFDokument4 Seitenmkl014 PDFFirdausFabriceHannanuNoch keine Bewertungen
- Tetanus PDFDokument11 SeitenTetanus PDFDwi Andriyani NimanNoch keine Bewertungen
- Tetanus PDFDokument11 SeitenTetanus PDFDwi Andriyani NimanNoch keine Bewertungen
- Lest We Forget 18Dokument4 SeitenLest We Forget 18VergaaBellanyNoch keine Bewertungen
- Guidelines Tetanus 2011Dokument8 SeitenGuidelines Tetanus 2011Nina YuliNoch keine Bewertungen
- Photographing Injuries in The Acute Care SettingDokument14 SeitenPhotographing Injuries in The Acute Care SettingVergaaBellanyNoch keine Bewertungen
- Lest We Forget 18Dokument4 SeitenLest We Forget 18VergaaBellanyNoch keine Bewertungen
- Table 4 19 1 - Tetanus Prophylaxis in Wound Management PDFDokument1 SeiteTable 4 19 1 - Tetanus Prophylaxis in Wound Management PDFVergaaBellanyNoch keine Bewertungen
- USG & Radiography in Detection of Hemothorax (2016)Dokument11 SeitenUSG & Radiography in Detection of Hemothorax (2016)VergaaBellanyNoch keine Bewertungen
- Tetanus ProfilaksisDokument4 SeitenTetanus ProfilaksisVergaaBellanyNoch keine Bewertungen
- Management of Haemothorax (1996) PDFDokument2 SeitenManagement of Haemothorax (1996) PDFVergaaBellanyNoch keine Bewertungen
- WHO - Haemoglobin Level For Anemia 2011Dokument6 SeitenWHO - Haemoglobin Level For Anemia 2011Adhi SanjayaNoch keine Bewertungen
- Abdominal Incisions and Sutures in Obstetrics and GynaecologyDokument6 SeitenAbdominal Incisions and Sutures in Obstetrics and GynaecologyFebyan AbotNoch keine Bewertungen
- Amckd Nice Guideline v8.1Dokument36 SeitenAmckd Nice Guideline v8.1vasarhely imolaNoch keine Bewertungen
- Mental Diseases and Criminal Offences Commited by Persons Placed at The Forensic DepartmentDokument7 SeitenMental Diseases and Criminal Offences Commited by Persons Placed at The Forensic DepartmentVergaaBellanyNoch keine Bewertungen
- Ssti PDFDokument4 SeitenSsti PDFflori.bNoch keine Bewertungen
- QuantAssay Software Manual 11-Mar-2019Dokument51 SeitenQuantAssay Software Manual 11-Mar-2019LykasNoch keine Bewertungen
- Class 12 - Maths - MatricesDokument87 SeitenClass 12 - Maths - MatricesAishwarya MishraNoch keine Bewertungen
- Vehicle Intercom Systems (VIS)Dokument4 SeitenVehicle Intercom Systems (VIS)bbeisslerNoch keine Bewertungen
- Lc420euf Sda1 LGDokument41 SeitenLc420euf Sda1 LGjavierNoch keine Bewertungen
- John Sisler CISSP Study GuideDokument126 SeitenJohn Sisler CISSP Study GuideAnthonyNoch keine Bewertungen
- Overall Method StatementDokument33 SeitenOverall Method Statementsaranga100% (1)
- Tsel Manual ThermoselDokument25 SeitenTsel Manual ThermoselPedro AlvelaisNoch keine Bewertungen
- Mullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorDokument15 SeitenMullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorKadag LhundrupNoch keine Bewertungen
- Material Requirement Planning (MRP)Dokument55 SeitenMaterial Requirement Planning (MRP)Lisa CarlsonNoch keine Bewertungen
- SCIENCEEEEEDokument3 SeitenSCIENCEEEEEChristmae MaganteNoch keine Bewertungen
- Texto CuritibaDokument1 SeiteTexto CuritibaMargarida GuimaraesNoch keine Bewertungen
- Latihan To: Nilai: 7.4 Benar: 37 Salah: 13Dokument17 SeitenLatihan To: Nilai: 7.4 Benar: 37 Salah: 13glensNoch keine Bewertungen
- Egt Margen From The Best ArticalDokument6 SeitenEgt Margen From The Best ArticalakeelNoch keine Bewertungen
- Chemical Bonds WorksheetDokument2 SeitenChemical Bonds WorksheetJewel Mae MercadoNoch keine Bewertungen
- Smoldering Combustion: Guillermo ReinDokument20 SeitenSmoldering Combustion: Guillermo ReinAhmed HussainNoch keine Bewertungen
- (Eng) Zx890lch 5a Ks En316Dokument13 Seiten(Eng) Zx890lch 5a Ks En316MC TAK LEENoch keine Bewertungen
- Electrical Power System Device Function NumberDokument2 SeitenElectrical Power System Device Function Numberdan_teegardenNoch keine Bewertungen
- ASCE Snow Loads On Solar-Paneled RoofsDokument61 SeitenASCE Snow Loads On Solar-Paneled RoofsBen100% (1)
- SAT Biochar Ethylene Poster 10 - 10b PDFDokument1 SeiteSAT Biochar Ethylene Poster 10 - 10b PDFsherifalharamNoch keine Bewertungen
- Modern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaDokument2 SeitenModern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaKumar KumarNoch keine Bewertungen
- Aircraft Design Course PhillStocking 4.2Dokument48 SeitenAircraft Design Course PhillStocking 4.2ugurugur1982Noch keine Bewertungen
- Guidelines For The Management of Brain InjuryDokument26 SeitenGuidelines For The Management of Brain InjuryfathaNoch keine Bewertungen
- 7 +Royal+Court+Affairs,+Sultanate+of+OmanDokument12 Seiten7 +Royal+Court+Affairs,+Sultanate+of+OmanElencheliyan PandeeyanNoch keine Bewertungen
- Full Download Short Term Financial Management 3rd Edition Maness Test BankDokument35 SeitenFull Download Short Term Financial Management 3rd Edition Maness Test Bankcimanfavoriw100% (31)
- Rac Question PaperDokument84 SeitenRac Question PaperibrahimNoch keine Bewertungen
- iPQ-Center Webvideo Star TTB MA R1 42 en PDFDokument32 SeiteniPQ-Center Webvideo Star TTB MA R1 42 en PDFHamid KharazmiNoch keine Bewertungen
- Binder 3 of 4 Dec-2018Dokument1.169 SeitenBinder 3 of 4 Dec-2018Anonymous OEmUQuNoch keine Bewertungen
- Chapter Three: 1 - The Coarse Grain SoilsDokument21 SeitenChapter Three: 1 - The Coarse Grain SoilsSalih MohayaddinNoch keine Bewertungen
- Properties of Matter ReviewDokument8 SeitenProperties of Matter Reviewapi-290100812Noch keine Bewertungen
- Hurricanes Grade5Dokument3 SeitenHurricanes Grade5Anonymous m3yrUPNoch keine Bewertungen