Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Genjrl 1Dokument1 SeiteGenjrl 1Tiara AjaNoch keine Bewertungen
- Procter & Gamble: Expansion PlanDokument6 SeitenProcter & Gamble: Expansion PlanSarthak AgarwalNoch keine Bewertungen
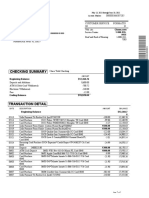
- Estado Bancario ChaseDokument2 SeitenEstado Bancario ChasePedro Ant. Núñez Ulloa100% (1)
- Chapter 3 & 4 Banking An Operations 2Dokument15 SeitenChapter 3 & 4 Banking An Operations 2ManavAgarwalNoch keine Bewertungen
- The Trap Sir James Goldsmith PDFDokument189 SeitenThe Trap Sir James Goldsmith PDFBob L100% (1)
- Fa Ii. ObjDokument5 SeitenFa Ii. ObjSonia ShamsNoch keine Bewertungen
- Taxation Reviewer - SAN BEDADokument128 SeitenTaxation Reviewer - SAN BEDAMark Lawrence Guzman93% (28)
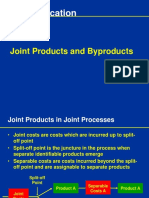
- Joint Cost Allocation Methods for Multiple ProductsDokument17 SeitenJoint Cost Allocation Methods for Multiple ProductsATLASNoch keine Bewertungen
- SAMPLEX A - Obligations and Contracts - Atty. Sta. Maria - Finals 2014Dokument2 SeitenSAMPLEX A - Obligations and Contracts - Atty. Sta. Maria - Finals 2014Don Dela ChicaNoch keine Bewertungen
- The Economic ProblemDokument22 SeitenThe Economic ProblemPeterNoch keine Bewertungen
- ReSA B45 AUD First PB Exam - Questions, Answers - SolutionsDokument21 SeitenReSA B45 AUD First PB Exam - Questions, Answers - SolutionsDhainne Enriquez100% (1)
- GRI 3: Material Topics 2021: Universal StandardDokument30 SeitenGRI 3: Material Topics 2021: Universal StandardMaría Belén MartínezNoch keine Bewertungen
- HDFC Standard Life Insurance Company-Recruitment and SelectionDokument74 SeitenHDFC Standard Life Insurance Company-Recruitment and Selectionindia2000050% (2)
- MELC - EPP 5 Entrep ICT MELCDokument2 SeitenMELC - EPP 5 Entrep ICT MELCChristian GranadaNoch keine Bewertungen
- Orange Book 2nd Edition 2011 AddendumDokument4 SeitenOrange Book 2nd Edition 2011 AddendumAlex JeavonsNoch keine Bewertungen
- SADIF-Investment AnalyticsDokument12 SeitenSADIF-Investment AnalyticsTony ZhangNoch keine Bewertungen
- Review of Related LiteratureDokument3 SeitenReview of Related LiteratureEaster Joy PatuladaNoch keine Bewertungen
- Greeting Card Business PlanDokument52 SeitenGreeting Card Business PlanChuck Achberger50% (2)
- Running Head: Ethical and Legal Principles On British AirwaysDokument8 SeitenRunning Head: Ethical and Legal Principles On British AirwaysDyya EllenaNoch keine Bewertungen
- Squash StickDokument56 SeitenSquash StickDanah Jane GarciaNoch keine Bewertungen
- ALIGNINGDokument16 SeitenALIGNINGgianlucaNoch keine Bewertungen
- IKEA PresentationDokument20 SeitenIKEA PresentationAvinash2458Noch keine Bewertungen
- BOI - New LetterDokument5 SeitenBOI - New Lettersandip_banerjeeNoch keine Bewertungen
- Benefits of MYOB Accounting SoftwareDokument13 SeitenBenefits of MYOB Accounting SoftwareTuba MirzaNoch keine Bewertungen
- Canons of TaxationDokument2 SeitenCanons of Taxationmadeeha_2475% (4)
- BASIC ACCOUNTING - PARTNERSHIP ADMISSIONSDokument26 SeitenBASIC ACCOUNTING - PARTNERSHIP ADMISSIONSVincent Larrie MoldezNoch keine Bewertungen
- 14 A Study On Women Empowerment Through Self Help Groups in IndiaDokument6 Seiten14 A Study On Women Empowerment Through Self Help Groups in IndiaPARAMASIVAN CHELLIAH100% (1)
- Unit 3 Assignment: A Simple BudgetDokument5 SeitenUnit 3 Assignment: A Simple BudgetNguyên KhánhNoch keine Bewertungen
- Budget LineDokument6 SeitenBudget Linegyan|_vermaNoch keine Bewertungen
- Accenture Service Design Tale Two Coffee Shops TranscriptDokument2 SeitenAccenture Service Design Tale Two Coffee Shops TranscriptAmilcar Alvarez de LeonNoch keine Bewertungen