Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Advances in The Management of Persistent Pain.110Dokument5 SeitenAdvances in The Management of Persistent Pain.110EmaDiaconuNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hand Hygiene Handout PDFDokument32 SeitenHand Hygiene Handout PDFms RN100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- WWW - Nbe.edu - In: Click Here For NEET-PG 2017 All India 50% Quota Result-Cum-Score CordDokument3 SeitenWWW - Nbe.edu - In: Click Here For NEET-PG 2017 All India 50% Quota Result-Cum-Score CordNixon GoyalNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- UniKl 171114 PDFDokument1 SeiteUniKl 171114 PDFCokelat KingNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Pharmacology Quiz Question & Answers (Question Bank) - 3Dokument1 SeitePharmacology Quiz Question & Answers (Question Bank) - 3Owusuasare ChrispakNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Talking With Voices-Learning From The DialogueDokument3 SeitenTalking With Voices-Learning From The DialogueGateway ProjectNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Final Examination in Mapeh 10 NewDokument2 SeitenFinal Examination in Mapeh 10 Newjennalyn Gabuya100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
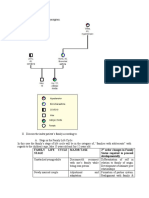
- Family Life Cycle Stage Major Task 2 Order Changes in Family Status Required To Proceed DevelopmentallyDokument6 SeitenFamily Life Cycle Stage Major Task 2 Order Changes in Family Status Required To Proceed DevelopmentallyAris Jasper NacionNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- NCP (Icu)Dokument2 SeitenNCP (Icu)jessie_nuñez_263% (8)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Referral FormDokument2 SeitenReferral Formraad_alghamdi_1Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Ebook Obstetrics Gynecology Morning Report Beyond The Pearls PDF Full Chapter PDFDokument67 SeitenEbook Obstetrics Gynecology Morning Report Beyond The Pearls PDF Full Chapter PDFsusan.perez986100% (27)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Health Assessment FormDokument2 SeitenHealth Assessment FormJessa MaeNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Jacynda Oun - ResumeDokument3 SeitenJacynda Oun - Resumeapi-281022713Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- CHN NCP Group 1 Docx Final PromiseDokument6 SeitenCHN NCP Group 1 Docx Final PromiseLeo Buquiran AcabalNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Self Study Report: 1 Cycle of AccreditationDokument120 SeitenSelf Study Report: 1 Cycle of AccreditationSatya AsatyaNoch keine Bewertungen
- Medicare Healthcare Sales Executive in CA Resume Bren WhitakerDokument2 SeitenMedicare Healthcare Sales Executive in CA Resume Bren Whitakerbefoundjobs613Noch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Nutrition Executive (Kuala Lumpur, Penang) Job - Danone Dumex (M) SDN BHD - 3789767 - JobStreetDokument3 SeitenNutrition Executive (Kuala Lumpur, Penang) Job - Danone Dumex (M) SDN BHD - 3789767 - JobStreetFiona LeongNoch keine Bewertungen
- Infliximab: Drug Treatment InformationDokument7 SeitenInfliximab: Drug Treatment InformationAlin-Ionuț SălcianuNoch keine Bewertungen
- Brachytherapy To Treat CancerDokument2 SeitenBrachytherapy To Treat CancerCrissel Kane CarpioNoch keine Bewertungen
- Fluid Therapy and ShockDokument8 SeitenFluid Therapy and ShockJuan Francisco SánchezNoch keine Bewertungen
- CHP Manual EN-webfinal PDFDokument29 SeitenCHP Manual EN-webfinal PDFmajaklipaNoch keine Bewertungen
- List Jurnal Scopus - Public Health, Environmental and Occupational HealthDokument41 SeitenList Jurnal Scopus - Public Health, Environmental and Occupational HealthindiraDLNoch keine Bewertungen
- Form PEMERIKSANAAN UMUM FT ANAK 300419Dokument4 SeitenForm PEMERIKSANAAN UMUM FT ANAK 300419vanoNoch keine Bewertungen
- C.S.lewis-Sfaturile Unui Diavol Batran Catre Unul Mai TanarDokument2 SeitenC.S.lewis-Sfaturile Unui Diavol Batran Catre Unul Mai TanarAdelina IştocNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Assessment Nursing Diagnosis Outcome Identification Planning Intervention Rationale Evaluation Subjective Data: Short Term: IndependentDokument2 SeitenAssessment Nursing Diagnosis Outcome Identification Planning Intervention Rationale Evaluation Subjective Data: Short Term: IndependentDimple Castañeto Callo100% (1)
- New Patient Registration Form TemplateDokument8 SeitenNew Patient Registration Form TemplateHasfi YakobNoch keine Bewertungen
- The Illinois Acupuncturist: Asian Moon Festival 2011Dokument28 SeitenThe Illinois Acupuncturist: Asian Moon Festival 2011Yiu Ming HuynhNoch keine Bewertungen
- Of The Secretary: OfficeDokument59 SeitenOf The Secretary: OfficeJoanna MarieNoch keine Bewertungen
- An Assessment of Manual Medical Record System of Fr. Simpliciano Academy Inc. School Year 2018-2019Dokument66 SeitenAn Assessment of Manual Medical Record System of Fr. Simpliciano Academy Inc. School Year 2018-2019Dimple SalesNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Practical Approach To Ethical Decision MakingDokument5 SeitenA Practical Approach To Ethical Decision MakingEmmy IsaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)