Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 5V To 48V DC Converter For Phantom Power Supplies - Full DIY Project PDFDokument3 Seiten5V To 48V DC Converter For Phantom Power Supplies - Full DIY Project PDFAbdul NoorNoch keine Bewertungen
- Enhanced Hybrid English 10 Q1 M2Dokument13 SeitenEnhanced Hybrid English 10 Q1 M2VNoch keine Bewertungen
- Bexley Selection Tests Specimen Questions - Verbal ReasoningDokument8 SeitenBexley Selection Tests Specimen Questions - Verbal Reasoningpflora41Noch keine Bewertungen
- Transport System Question and AnswersDokument12 SeitenTransport System Question and Answerskumara guruparanNoch keine Bewertungen
- Nielsen Shopper Insights - Retailers Segment - Client 051115 PDFDokument63 SeitenNielsen Shopper Insights - Retailers Segment - Client 051115 PDFn0isyb0yNoch keine Bewertungen
- Diagnostic CentreDokument66 SeitenDiagnostic CentreMoolam RaoNoch keine Bewertungen
- Determination of Fat (Food Analysis)Dokument7 SeitenDetermination of Fat (Food Analysis)Nabila Husna100% (2)
- Biological Molecules Notes o LevelDokument10 SeitenBiological Molecules Notes o LevelFangsNoch keine Bewertungen
- Lesson 2 Professionals and Practitioners in CounselingDokument93 SeitenLesson 2 Professionals and Practitioners in CounselingDaneNoch keine Bewertungen
- Exercise 1. QuantifiersDokument1 SeiteExercise 1. QuantifiersIrynaNoch keine Bewertungen
- Ngo PrimaDokument11 SeitenNgo PrimaAleksandar BačlijaNoch keine Bewertungen
- Behavioral Economics - Problem Set 1Dokument4 SeitenBehavioral Economics - Problem Set 1Evans LoveNoch keine Bewertungen
- H2S Scrubber SpecificationDokument1 SeiteH2S Scrubber SpecificationKapwell LimitedNoch keine Bewertungen
- Relationship between cytokines and hazards in waste workersDokument8 SeitenRelationship between cytokines and hazards in waste workersSalsa BilaNoch keine Bewertungen
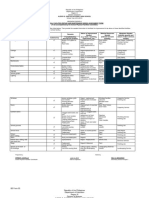
- Brigada Eskwela Forms 1 and 3Dokument4 SeitenBrigada Eskwela Forms 1 and 3Mar Sebastian100% (1)
- QUES3Dokument10 SeitenQUES3Múrtåzâ LãxmīdhârNoch keine Bewertungen
- SVM-7600 Series Bedside Monitor Advanced Monitoring and ReviewDokument4 SeitenSVM-7600 Series Bedside Monitor Advanced Monitoring and ReviewCathy Palongpong TumaraoNoch keine Bewertungen
- Chapter 03 The Eye and RetinaDokument10 SeitenChapter 03 The Eye and RetinaSimrat WNoch keine Bewertungen
- Dog Training Book Rex in The CityDokument56 SeitenDog Training Book Rex in The CitybebekbuluhNoch keine Bewertungen
- Key Areas of Risk For Woolworths Ltd.Dokument19 SeitenKey Areas of Risk For Woolworths Ltd.Allison BestNoch keine Bewertungen
- G8 en La Evaluación GeriátricaDokument12 SeitenG8 en La Evaluación GeriátricaMIGUEL MORENONoch keine Bewertungen
- IGA Report FINAL 10 07 2016Dokument171 SeitenIGA Report FINAL 10 07 2016Timothy SchwartzNoch keine Bewertungen
- Promotion of Tax Culture in Pakistan: Perspective, Prospects and ChallengesDokument5 SeitenPromotion of Tax Culture in Pakistan: Perspective, Prospects and ChallengesRaheel JoyiaNoch keine Bewertungen
- Chemical and Enzymatic Synthesis of LanthioninesDokument15 SeitenChemical and Enzymatic Synthesis of LanthioninesSam SonNoch keine Bewertungen
- People V Veneracion Case DigestDokument3 SeitenPeople V Veneracion Case DigestraykarloBNoch keine Bewertungen
- Chemistry ProjectDokument11 SeitenChemistry ProjectEktaMallikNoch keine Bewertungen
- Cell Cycle DisordersDokument22 SeitenCell Cycle DisordersFatima IffatNoch keine Bewertungen
- 02 - Motor PDFDokument80 Seiten02 - Motor PDFRenato Assis da SilvaNoch keine Bewertungen
- Definition, Limits and Agents of MetamorphismDokument13 SeitenDefinition, Limits and Agents of MetamorphismSajid IqrarNoch keine Bewertungen
- Chemical Engineering Science: Ishara Dedunu Kamalanathan, Peter James MartinDokument11 SeitenChemical Engineering Science: Ishara Dedunu Kamalanathan, Peter James MartinarulrajasiNoch keine Bewertungen