Das könnte Ihnen auch gefallen
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- The Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandThe Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- The FRCS Exam Experience Gopikanthan ManoharanDokument5 SeitenThe FRCS Exam Experience Gopikanthan Manoharanasi basseyNoch keine Bewertungen
- Pod EssentialDokument60 SeitenPod EssentialAmar AlkhafajiNoch keine Bewertungen
- @MedicalBooksStore 2013 ExternalDokument431 Seiten@MedicalBooksStore 2013 ExternalОлександр ШендераNoch keine Bewertungen
- Postgraduate Orthopaedics Viva Guide For The Frcs TR Orth ExaminationDokument29 SeitenPostgraduate Orthopaedics Viva Guide For The Frcs TR Orth ExaminationAshish Batra0% (1)
- Tennis ElbowDokument13 SeitenTennis ElbowPadma PadalNoch keine Bewertungen
- Gpe - 017.1 - Orthopaedic ExaminationDokument3 SeitenGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumNoch keine Bewertungen
- PreviewDokument24 SeitenPreviewSabryNoch keine Bewertungen
- 2004, Vol.23, Issues 1, Athletic Foot and Ankle InjuriesDokument165 Seiten2004, Vol.23, Issues 1, Athletic Foot and Ankle InjuriesAndrei Gianina100% (3)
- Practical ProceduresDokument315 SeitenPractical ProceduresAnil SoodNoch keine Bewertungen
- Alingment in TKRDokument3 SeitenAlingment in TKRdeepak100% (1)
- OKU Referat Bedah PDFDokument469 SeitenOKU Referat Bedah PDFAde ZulfiahNoch keine Bewertungen
- Topic Wise DNB Papers OrthoDokument53 SeitenTopic Wise DNB Papers OrthoKirubakaran Saraswathy PattabiramanNoch keine Bewertungen
- Mukharjee Regimen 321Dokument16 SeitenMukharjee Regimen 321shreyahospital.motinagarNoch keine Bewertungen
- AAOS2012 Foot and AnkleDokument103 SeitenAAOS2012 Foot and AnkleAmmar HilliNoch keine Bewertungen
- @ankle BreakerDokument2 Seiten@ankle BreakerEGNoch keine Bewertungen
- Queens Orthopedic Inpatient Trauma PDFDokument27 SeitenQueens Orthopedic Inpatient Trauma PDFRema AmerNoch keine Bewertungen
- Osce Grand RoundDokument32 SeitenOsce Grand Rounddoos1Noch keine Bewertungen
- Foot and Ankle Anatomy and Physical Examination PART 1Dokument49 SeitenFoot and Ankle Anatomy and Physical Examination PART 1eric sivaneshNoch keine Bewertungen
- AO-OTA Pelvis Fracture ClassificationDokument5 SeitenAO-OTA Pelvis Fracture ClassificationSyed Al100% (1)
- Handbook of Foot and Ankle Orthopedics (Rational Prescription of Foot and Ankle Orthotics) PDFDokument6 SeitenHandbook of Foot and Ankle Orthopedics (Rational Prescription of Foot and Ankle Orthotics) PDFAbdallah Jaber100% (2)
- Trauma & Orthopaedic SurgeryDokument120 SeitenTrauma & Orthopaedic SurgeryOstazNoch keine Bewertungen
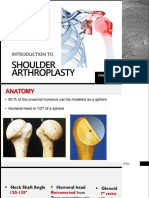
- KHA Shoulder Arthroplasty FinalDokument27 SeitenKHA Shoulder Arthroplasty FinalKyaw Htet Aung100% (1)
- Coughlin & MannDokument4.539 SeitenCoughlin & MannNicholas CampitelliNoch keine Bewertungen
- Orthopaedics PunchDokument6 SeitenOrthopaedics PunchHicham GawishNoch keine Bewertungen
- Operative Techniques in Orthopaedic Surgery - 2nd - Distal Chevron OsteotomyDokument15 SeitenOperative Techniques in Orthopaedic Surgery - 2nd - Distal Chevron OsteotomyakaandykayNoch keine Bewertungen
- Common CasesDokument44 SeitenCommon CasesRebecca WongNoch keine Bewertungen
- Crozer-Keystone Ex Tern Ship ManualDokument187 SeitenCrozer-Keystone Ex Tern Ship ManualRihamary CruzNoch keine Bewertungen
- Management of The Floating Knee.Dokument8 SeitenManagement of The Floating Knee.barbara liuva chia policarpoNoch keine Bewertungen
- Distal Femur (Sandeep Sir)Dokument22 SeitenDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNoch keine Bewertungen
- Ilizarov Fixator: DR Pratik AgarwalDokument86 SeitenIlizarov Fixator: DR Pratik AgarwaltesfahuntekletilahunNoch keine Bewertungen
- Plastic Surgery For Trauma The Essential Survival Guide (Dorian Hobday, Ted Welman, Max Horwitz Etc.) (Z-Library)Dokument233 SeitenPlastic Surgery For Trauma The Essential Survival Guide (Dorian Hobday, Ted Welman, Max Horwitz Etc.) (Z-Library)Cosa Catalin100% (1)
- Guide To Trauma and Orthopaedics in SWTDokument14 SeitenGuide To Trauma and Orthopaedics in SWTapi-276370510Noch keine Bewertungen
- Ankle Arthrodesis - Screw FixationDokument26 SeitenAnkle Arthrodesis - Screw FixationChristopher HoodNoch keine Bewertungen
- Antibacterial Cheat SheatDokument1 SeiteAntibacterial Cheat Sheatnkarimova2Noch keine Bewertungen
- Orthopedics LogbookDokument7 SeitenOrthopedics LogbookvishalzeniaNoch keine Bewertungen
- AO-ASIF - Instruments & ImplantsDokument582 SeitenAO-ASIF - Instruments & ImplantsthiagoNoch keine Bewertungen
- Accordion Maneuver - A Bloodless Tool in IlizarovDokument5 SeitenAccordion Maneuver - A Bloodless Tool in Ilizarovsheshagiri vNoch keine Bewertungen
- Syllabus Ms OrthoDokument8 SeitenSyllabus Ms OrthoMuthu KumarNoch keine Bewertungen
- 2016 OITE Study Guide For ResidentsDokument273 Seiten2016 OITE Study Guide For Residentschu_chiang_3100% (1)
- Fractures and Dislocations About The Elbow in The Pediatric PatientDokument65 SeitenFractures and Dislocations About The Elbow in The Pediatric PatientPeter HubkaNoch keine Bewertungen
- Pediatric Bone TumorsDokument20 SeitenPediatric Bone TumorsFelipe VenegasNoch keine Bewertungen
- 20 Orthopedic EmergenciesDokument48 Seiten20 Orthopedic Emergenciesfzee13Noch keine Bewertungen
- Clinical Examination of The Wrist PDFDokument11 SeitenClinical Examination of The Wrist PDFAdosotoNoch keine Bewertungen
- Tureks Orthopaedics - Principles and Their ApplicDokument1 SeiteTureks Orthopaedics - Principles and Their Applicqu402113Noch keine Bewertungen
- Orthopaedic EssaysDokument139 SeitenOrthopaedic EssaysDuncan Jackson100% (1)
- Total Knee Replacement: The Path ToDokument6 SeitenTotal Knee Replacement: The Path ToMoses DhinakarNoch keine Bewertungen
- BooksDokument1 SeiteBooksAnonymous atS3ugNoch keine Bewertungen
- OITE 2006 Questions For Nyssh UpdateDokument31 SeitenOITE 2006 Questions For Nyssh UpdateICH KhuyNoch keine Bewertungen
- Bone Transport Distraction Osteogenesis 1Dokument31 SeitenBone Transport Distraction Osteogenesis 1Euginia YosephineNoch keine Bewertungen
- Orthopedics: Notes, 1/eDokument26 SeitenOrthopedics: Notes, 1/evkNoch keine Bewertungen
- Tennis Elbow JOSPT ArticleDokument11 SeitenTennis Elbow JOSPT ArticleHasan RahmanNoch keine Bewertungen
- Arthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.Dokument12 SeitenArthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.C Martin TraumatoNoch keine Bewertungen
- Ankle and Foot Examination PDFDokument16 SeitenAnkle and Foot Examination PDFainizatiNoch keine Bewertungen
- Hand OITE - 2012 2013 2014Dokument209 SeitenHand OITE - 2012 2013 2014Sadiq AliNoch keine Bewertungen
- Ortho Xray MeasurmentsDokument110 SeitenOrtho Xray MeasurmentsPriza RazunipNoch keine Bewertungen
- MODIFIED POSTERIOR APPROACH TO THE HIP JOINTVon EverandMODIFIED POSTERIOR APPROACH TO THE HIP JOINTBewertung: 5 von 5 Sternen5/5 (1)
- Posterior Cruciate Ligament Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandPosterior Cruciate Ligament Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Bone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsVon EverandBone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsNoch keine Bewertungen
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Dokument3 SeitenLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyeNoch keine Bewertungen
- READMEDokument1 SeiteREADMETyler Lawrence CoyeNoch keine Bewertungen
- Meta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingDokument21 SeitenMeta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingTyler Lawrence CoyeNoch keine Bewertungen
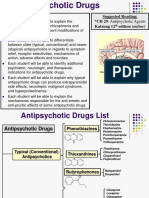
- AntipsychoticsDokument29 SeitenAntipsychoticsTyler Lawrence Coye100% (5)
- Lecture 3 Capsule Tendon Balance ProceduresDokument19 SeitenLecture 3 Capsule Tendon Balance ProceduresTyler Lawrence CoyeNoch keine Bewertungen
- Treatment of Lisfranc Fracture-Dislocations With PDokument8 SeitenTreatment of Lisfranc Fracture-Dislocations With PTyler Lawrence CoyeNoch keine Bewertungen
- Penn Presby Residency Manual PodiatryDokument400 SeitenPenn Presby Residency Manual PodiatryTyler Lawrence Coye100% (1)
- Lecture-12-2 22 17Dokument7 SeitenLecture-12-2 22 17Tyler Lawrence CoyeNoch keine Bewertungen
- 16 Principles of Ankle and Foot CTDokument48 Seiten16 Principles of Ankle and Foot CTTyler Lawrence CoyeNoch keine Bewertungen
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDokument16 SeitenThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- AnticoagulantsDokument47 SeitenAnticoagulantsTyler Lawrence Coye100% (1)
- Wound and Skin Ulcer Management Care Guide PDFDokument21 SeitenWound and Skin Ulcer Management Care Guide PDFAdriel Chandra AngNoch keine Bewertungen
- Respratory Drugs I-IIDokument10 SeitenRespratory Drugs I-IITyler Lawrence CoyeNoch keine Bewertungen
- Crozer Manual - Second Edition PDFDokument219 SeitenCrozer Manual - Second Edition PDFTyler Lawrence CoyeNoch keine Bewertungen
- Anatomy RecallDokument337 SeitenAnatomy RecallTyler Lawrence Coye100% (2)
- Drugs Class Mechanism: Guaifenesin (OTC)Dokument10 SeitenDrugs Class Mechanism: Guaifenesin (OTC)Tyler Lawrence CoyeNoch keine Bewertungen
- Goljan Step 1 HY 36 Pages Notes PDFDokument36 SeitenGoljan Step 1 HY 36 Pages Notes PDFTyler Lawrence CoyeNoch keine Bewertungen
- Reaction Notes For Organic ChemistryDokument11 SeitenReaction Notes For Organic ChemistryTyler Lawrence CoyeNoch keine Bewertungen
- Tercera SemanaDokument9 SeitenTercera SemanaJesús Torres MayaNoch keine Bewertungen
- CEBM Diagnostic Study Appraisal WorksheetDokument3 SeitenCEBM Diagnostic Study Appraisal WorksheetNur RifqahNoch keine Bewertungen
- Understanding The RelapseDokument12 SeitenUnderstanding The RelapseruziyanaNoch keine Bewertungen
- Ncbi List of Books and Dental ArticlesDokument6 SeitenNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- CBDRP Reporting Form 1Dokument1 SeiteCBDRP Reporting Form 1Romer EnajeNoch keine Bewertungen
- EMR Documentation TemplatesDokument25 SeitenEMR Documentation TemplatesFlint Ray100% (1)
- Gastritis, Deodenitis and Bleeding Deodenal Ulcer Following Mefenamic Acid TherapyDokument3 SeitenGastritis, Deodenitis and Bleeding Deodenal Ulcer Following Mefenamic Acid TherapyAimanul H.Noch keine Bewertungen
- 1.0 Thrombocytes SCDokument10 Seiten1.0 Thrombocytes SC西矢椛Noch keine Bewertungen
- The Conceptual Evolution of DSM 5Dokument391 SeitenThe Conceptual Evolution of DSM 5monkey85222100% (3)
- WEVM Chapter 1Dokument22 SeitenWEVM Chapter 1Manoj KarkiNoch keine Bewertungen
- Axa Group Corporate PresentationDokument35 SeitenAxa Group Corporate PresentationRajneesh VermaNoch keine Bewertungen
- Chest Pain FinalDokument17 SeitenChest Pain FinalVarun R'MenonNoch keine Bewertungen
- Preeclampsia Nursing Care PlanDokument5 SeitenPreeclampsia Nursing Care PlanBSN 3-2 RUIZ, Jewel Anne F.Noch keine Bewertungen
- Sheet 2 (Local Anesthesia 2)Dokument14 SeitenSheet 2 (Local Anesthesia 2)ardesh abdilleNoch keine Bewertungen
- Prevalence and Determinants of Substance Use Among Students at Kampala International University Western Campus, Ishaka Municipality Bushenyi District UgandaDokument18 SeitenPrevalence and Determinants of Substance Use Among Students at Kampala International University Western Campus, Ishaka Municipality Bushenyi District UgandaKIU PUBLICATION AND EXTENSIONNoch keine Bewertungen
- Aneurysm: Symptoms of An AneurysmDokument3 SeitenAneurysm: Symptoms of An AneurysmArun MuralidharanNoch keine Bewertungen
- Icru 89 (229-260)Dokument32 SeitenIcru 89 (229-260)Christian Ordoñez100% (1)
- Mental IllnessDokument3 SeitenMental IllnessKate EvangelistaNoch keine Bewertungen
- University of Zimbabwe Dissertation TopicsDokument4 SeitenUniversity of Zimbabwe Dissertation TopicsCustomWritingPaperServiceCanada100% (1)
- Modifiers-Table 122015 2Dokument25 SeitenModifiers-Table 122015 2khatNoch keine Bewertungen
- Celiac DiseaseDokument5 SeitenCeliac DiseaseJhevey ValdezNoch keine Bewertungen
- OlanzapineDokument1 SeiteOlanzapineKallie ChartrandNoch keine Bewertungen
- Massage Techniques and Effects PresentationDokument35 SeitenMassage Techniques and Effects Presentationama00Noch keine Bewertungen
- Vitamin and Mineral Supplementation During PregnanDokument4 SeitenVitamin and Mineral Supplementation During PregnanEvi RachmawatiNoch keine Bewertungen
- Counseling TechniquesDokument60 SeitenCounseling Techniquesdinalen0% (1)
- Reflection Paper Pediatric Community-Acquired Pneumonia in The United StatesDokument2 SeitenReflection Paper Pediatric Community-Acquired Pneumonia in The United StatesLecery Sophia WongNoch keine Bewertungen
- Che 225 Control of Communicable DiseasesDokument19 SeitenChe 225 Control of Communicable DiseasesAbdullahi Bashir SalisuNoch keine Bewertungen
- Festival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Dokument29 SeitenFestival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Maria Fe VibarNoch keine Bewertungen
- Lipo LaserDokument13 SeitenLipo LaserLuis A Gil Pantoja100% (1)
- Full Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadDokument11 SeitenFull Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadFlip Body SpaNoch keine Bewertungen