Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Pathology+101 Complete)Dokument147 SeitenPathology+101 Complete)Goh Kah Yong100% (2)
- Renal QuizDokument2 SeitenRenal QuizJune Dumdumaya75% (4)
- Stoelting Anasthesia and Co Existing Disease PDFDokument28 SeitenStoelting Anasthesia and Co Existing Disease PDFEgidia SetyaNoch keine Bewertungen
- Osmosis Acute Coronary SyndromesDokument5 SeitenOsmosis Acute Coronary Syndromesvalentinabil3Noch keine Bewertungen
- Establishing The Mechanism of Supraventricular Tachycardia in The Electrophysiology LaboratoryDokument15 SeitenEstablishing The Mechanism of Supraventricular Tachycardia in The Electrophysiology LaboratorySamuelNoch keine Bewertungen
- p56 - p110Dokument6 Seitenp56 - p110Bhushan D ThombareNoch keine Bewertungen
- Inflamatory Heart DiseaseDokument42 SeitenInflamatory Heart DiseaseChalie MequanentNoch keine Bewertungen
- Queensland RMO Application GuideDokument18 SeitenQueensland RMO Application GuideSOMANATHAN UMAHSUTHANNoch keine Bewertungen
- 1 s2.0 S2772930322004367 MainDokument15 Seiten1 s2.0 S2772930322004367 MainVimal NishadNoch keine Bewertungen
- What Is Tetralogy of FallotDokument3 SeitenWhat Is Tetralogy of FallotJyedenn PonceNoch keine Bewertungen
- Systematic ReviewDokument10 SeitenSystematic ReviewLeeyaa CullenNoch keine Bewertungen
- Critical Care Intravenous Infusion Drug Handbook 3rd EditionDokument61 SeitenCritical Care Intravenous Infusion Drug Handbook 3rd Editionsharon.correia689100% (40)
- Facts About Sudden Cardiac ArrestDokument2 SeitenFacts About Sudden Cardiac ArrestZeljko LekovicNoch keine Bewertungen
- Left Anterior Fascicular Block (LAFB) ECG Review - Criteria and ExamplesDokument1 SeiteLeft Anterior Fascicular Block (LAFB) ECG Review - Criteria and ExamplesWiwik Puji LestariNoch keine Bewertungen
- Electrocardiogram: Dr. PacnaDokument13 SeitenElectrocardiogram: Dr. PacnaEcel AggasidNoch keine Bewertungen
- Renal FailureDokument23 SeitenRenal FailurerjfeeleyNoch keine Bewertungen
- Neacsu Aurelia EssayDokument3 SeitenNeacsu Aurelia EssaySimona NeacsuNoch keine Bewertungen
- 30947630Dokument12 Seiten30947630carolinapolotorresNoch keine Bewertungen
- Mindmap CVS Liana Naamnih Group3Dokument1 SeiteMindmap CVS Liana Naamnih Group3Liana NaamnehNoch keine Bewertungen
- Cardiopulmunary ResucitationDokument13 SeitenCardiopulmunary ResucitationRussel OlivoNoch keine Bewertungen
- VT Origin PDFDokument60 SeitenVT Origin PDFNikita PratamaNoch keine Bewertungen
- Module 1Dokument13 SeitenModule 1MaseaNoch keine Bewertungen
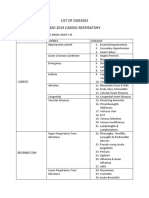
- List of Diseases Imo 2019 Cardio-RespiratoryDokument2 SeitenList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNoch keine Bewertungen
- Tatalaksana Hiperosmolar Hiperglicemic State (SHH)Dokument16 SeitenTatalaksana Hiperosmolar Hiperglicemic State (SHH)Vidya VidyutNoch keine Bewertungen
- End-Stage Renal DiseaseDokument7 SeitenEnd-Stage Renal Diseasemarvin de castroNoch keine Bewertungen
- Preoperative Cardiac Risk AssessmentDokument16 SeitenPreoperative Cardiac Risk Assessmentkrysmelis MateoNoch keine Bewertungen
- ACS-STEMI Management (Dr. Bambang Herwanto, SPJP)Dokument40 SeitenACS-STEMI Management (Dr. Bambang Herwanto, SPJP)Syafrinaldi JafrilNoch keine Bewertungen
- Nephrotic Syndrome: Akynbay MoldirDokument8 SeitenNephrotic Syndrome: Akynbay MoldirMoldir AkynbayNoch keine Bewertungen
- Beyond Wedge: Clinical Physiology and The Swan-Ganz CatheterDokument12 SeitenBeyond Wedge: Clinical Physiology and The Swan-Ganz Catheterkromatin9462Noch keine Bewertungen
- BCU 2022 First Announcement RevDokument14 SeitenBCU 2022 First Announcement RevAnggar KingStyle100% (1)