Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Community Assessment Ebi PaperDokument8 SeitenCommunity Assessment Ebi Paperapi-661765354Noch keine Bewertungen
- National Infection Control Guidelines - 2016 Draft For ConsultationDokument341 SeitenNational Infection Control Guidelines - 2016 Draft For Consultationlimiya vargheseNoch keine Bewertungen
- Central Venous Catheterization: Videos in Clinical MedicineDokument3 SeitenCentral Venous Catheterization: Videos in Clinical Medicineroy jeffry ancasi veraNoch keine Bewertungen
- Ultrasound-Guided Insertion of A Radial Arterial CatheterDokument4 SeitenUltrasound-Guided Insertion of A Radial Arterial CatheterNaomi RyuNoch keine Bewertungen
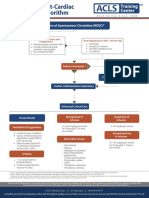
- Algo Postarrest PDFDokument1 SeiteAlgo Postarrest PDFdewita wahyu kemalasariNoch keine Bewertungen
- Algoritma BradycardiaDokument1 SeiteAlgoritma BradycardiaFiya SahrulNoch keine Bewertungen
- Circulatory ShockDokument9 SeitenCirculatory ShockTri UtomoNoch keine Bewertungen
- Lecture NotesDokument1 SeiteLecture NotesNaomi RyuNoch keine Bewertungen
- Seymour 2016Dokument13 SeitenSeymour 2016Arive Haruzz BizzaNoch keine Bewertungen
- Algoritma BradycardiaDokument1 SeiteAlgoritma BradycardiaFiya SahrulNoch keine Bewertungen
- Design and ImplementDokument1 SeiteDesign and ImplementNaomi RyuNoch keine Bewertungen
- Where States Stand On Medicaid Expansion Decisions - NASHPDokument2 SeitenWhere States Stand On Medicaid Expansion Decisions - NASHPNaomi RyuNoch keine Bewertungen
- Exercise 31 ECGHeartsoundsDokument11 SeitenExercise 31 ECGHeartsoundsNaomi Ryu100% (1)
- Jefferson On The Constitutionality of The BankDokument4 SeitenJefferson On The Constitutionality of The BankNaomi RyuNoch keine Bewertungen
- Practice Mcat 3: Ken Evans, MSC, MD Charlene Bramwell, MedDokument47 SeitenPractice Mcat 3: Ken Evans, MSC, MD Charlene Bramwell, MedNaomi RyuNoch keine Bewertungen
- Practice Mcat 3: Ken Evans, MSC, MD Charlene Bramwell, MedDokument47 SeitenPractice Mcat 3: Ken Evans, MSC, MD Charlene Bramwell, MedNaomi RyuNoch keine Bewertungen
- QuestionsDokument3 SeitenQuestionsNaomi RyuNoch keine Bewertungen
- AP Chap 18 19 HW Solutions CircuitsDokument22 SeitenAP Chap 18 19 HW Solutions CircuitsNaomi RyuNoch keine Bewertungen
- Racgp Combined Pdfs Single FileDokument1.983 SeitenRacgp Combined Pdfs Single FileVikrant100% (1)
- Ra 7277Dokument12 SeitenRa 7277KimAn 金安 PavonNoch keine Bewertungen
- Fall 2008 Wiley Consumer CatalogDokument102 SeitenFall 2008 Wiley Consumer CatalogNatalie Lin100% (17)
- ERF IMC3 IMC4 Evaluation ENGDokument4 SeitenERF IMC3 IMC4 Evaluation ENGNsabimana PatrickNoch keine Bewertungen
- MAPEH Health GR 10 Week 1 2Dokument18 SeitenMAPEH Health GR 10 Week 1 2vince bacaniNoch keine Bewertungen
- PEPFAR Country Operational Plane (COP) Guidance 2010 Programs - June 29 2009 FinalDokument147 SeitenPEPFAR Country Operational Plane (COP) Guidance 2010 Programs - June 29 2009 FinalAccessible Journal Media: Peace Corps DocumentsNoch keine Bewertungen
- MOHO with Adolescents & Adults with CancerDokument20 SeitenMOHO with Adolescents & Adults with CancerZahe'sNoch keine Bewertungen
- Chapter 1 3Dokument15 SeitenChapter 1 3Raymund T. Baño0% (1)
- Family Nursing ProcessDokument12 SeitenFamily Nursing ProcessChristine CornagoNoch keine Bewertungen
- Asnake TesfayeDokument232 SeitenAsnake TesfayeMohammed AbdiNoch keine Bewertungen
- Coronavirus Disease 2019 (COVID-19) - Cancer Screening, Diagnosis, Treatment, and Posttreatment Surveillance in Uninfected Patients During The Pandemic - UpToDateDokument55 SeitenCoronavirus Disease 2019 (COVID-19) - Cancer Screening, Diagnosis, Treatment, and Posttreatment Surveillance in Uninfected Patients During The Pandemic - UpToDateTatiana Valencia CastañoNoch keine Bewertungen
- Discharge Planning ProjectDokument6 SeitenDischarge Planning Projectapi-282958026Noch keine Bewertungen
- Capstone 2021 Paper Chi Nguyen FinaleditDokument19 SeitenCapstone 2021 Paper Chi Nguyen Finaleditapi-487551161Noch keine Bewertungen
- GAD Database DCFDokument26 SeitenGAD Database DCFBaby Jane Dedase100% (1)
- Lead Poisoning in Historical Perspective PDFDokument11 SeitenLead Poisoning in Historical Perspective PDFintan permata balqisNoch keine Bewertungen
- Professor Prisca Olabisi AdejumoDokument2 SeitenProfessor Prisca Olabisi AdejumoGodwin UgborNoch keine Bewertungen
- HEAL 2013 RecommendationsDokument39 SeitenHEAL 2013 RecommendationsDhawan SandeepNoch keine Bewertungen
- Curriculum Guide for Autism Primary Level 2 HealthDokument3 SeitenCurriculum Guide for Autism Primary Level 2 HealthXlian Myzter YosaNoch keine Bewertungen
- Alcohol Treatment CodesDokument3 SeitenAlcohol Treatment CodesMia JacksonNoch keine Bewertungen
- Art 20198412Dokument19 SeitenArt 20198412Nazneen AkhterNoch keine Bewertungen
- RN Role in Primary HealthcareDokument7 SeitenRN Role in Primary HealthcareNandia SeptiyoriniNoch keine Bewertungen
- J CDC RecommendationsDokument6 SeitenJ CDC RecommendationsmikeysiopaoNoch keine Bewertungen
- June, 2012 Jimma EthiopiaDokument32 SeitenJune, 2012 Jimma Ethiopianegussie birieNoch keine Bewertungen
- Indian Public Health Standards (IPHS) For Sub-Centres: DraftDokument60 SeitenIndian Public Health Standards (IPHS) For Sub-Centres: DraftRekha ChakrabartiNoch keine Bewertungen
- Stress at WorkplaceDokument10 SeitenStress at WorkplacesachnilaNoch keine Bewertungen
- University of Saint Louis Nursing Fundamentals ModuleDokument33 SeitenUniversity of Saint Louis Nursing Fundamentals ModuleAngelene CalivaNoch keine Bewertungen
- OVERVIEW of CHN Report Sir JOSEDokument7 SeitenOVERVIEW of CHN Report Sir JOSEVanessa Andrei Peralta CamelloNoch keine Bewertungen
- Indivdual Behavior: PPT PresentationDokument19 SeitenIndivdual Behavior: PPT PresentationDoll DollNoch keine Bewertungen