Das könnte Ihnen auch gefallen
- Texto guía para el diagnóstico y manejo del VIH en el embarazoVon EverandTexto guía para el diagnóstico y manejo del VIH en el embarazoNoch keine Bewertungen
- Oligohidramnios PDFDokument3 SeitenOligohidramnios PDFGerman Victoria0% (1)
- Shock Hipovolémico y EmbarazoDokument54 SeitenShock Hipovolémico y EmbarazoZony RiveraNoch keine Bewertungen
- Acog Transtornos Hipertensivos en El EmbarazoDokument25 SeitenAcog Transtornos Hipertensivos en El EmbarazoNashaly Pérez100% (4)
- Manual - Salvavidas ObstetricoDokument68 SeitenManual - Salvavidas ObstetricoCarol P Fernandez100% (3)
- Episiotomia Acog EspañolDokument28 SeitenEpisiotomia Acog EspañolDaniel I. Figueroa100% (1)
- Circulación Utero - Placentaria e Intercambio RespiratorioDokument59 SeitenCirculación Utero - Placentaria e Intercambio RespiratorioAry Gutiérrez100% (1)
- Recomendaciones Figo-Misoprostol SoloDokument5 SeitenRecomendaciones Figo-Misoprostol SolodoctorhackerNoch keine Bewertungen
- Maniobras de Parto PodálicoDokument2 SeitenManiobras de Parto PodálicoANGHY MIGUEL CAMPOSNoch keine Bewertungen
- Estudio de UrodinamiaDokument52 SeitenEstudio de UrodinamiaCarlos BarreraNoch keine Bewertungen
- ,protocolo de HisterectomíaDokument8 Seiten,protocolo de HisterectomíaYajaira AtiajaNoch keine Bewertungen
- Tarjetas Resumen GinecologíaDokument65 SeitenTarjetas Resumen GinecologíaFrapsssNoch keine Bewertungen
- Contusion Pulmonar.2Dokument17 SeitenContusion Pulmonar.2ed uardoNoch keine Bewertungen
- Pae Paciente Circunsicion de Pediatria 701 Janet Pacheco LaraDokument45 SeitenPae Paciente Circunsicion de Pediatria 701 Janet Pacheco LaraJM GarciaNoch keine Bewertungen
- Preeclampsia - Pathogenesis - UpToDateDokument42 SeitenPreeclampsia - Pathogenesis - UpToDateIngrid HolguinoNoch keine Bewertungen
- Sepsis 2020Dokument49 SeitenSepsis 2020Dariela0% (1)
- Shock Hipovolémico en ObstetriciaDokument28 SeitenShock Hipovolémico en ObstetriciaMayan King50% (6)
- Directrices de Tokio 2018Dokument15 SeitenDirectrices de Tokio 2018AnnelG RuizNoch keine Bewertungen
- Manejo de Masas AnexialesDokument5 SeitenManejo de Masas AnexialesjakiNoch keine Bewertungen
- Anatomia y Fisiologia de La Placenta InfografiaDokument1 SeiteAnatomia y Fisiologia de La Placenta Infografiabeto medinaNoch keine Bewertungen
- Algoritmo Distocias Mecanicas de Origen MaternoDokument5 SeitenAlgoritmo Distocias Mecanicas de Origen MaternoJoana MagallanesNoch keine Bewertungen
- Empozoñamiento Ofidico PDFDokument55 SeitenEmpozoñamiento Ofidico PDFMiguelBaezNoch keine Bewertungen
- Nals 2017Dokument174 SeitenNals 2017comida hawaina100% (1)
- 9 - Perfil Biofisico FetalDokument40 Seiten9 - Perfil Biofisico FetalYuri Cano Zirena75% (4)
- Monografia Anestesia Obstetrica Trabajo FinalDokument66 SeitenMonografia Anestesia Obstetrica Trabajo FinalHector Quilla0% (1)
- Trasnfusiones ObstetriciaDokument8 SeitenTrasnfusiones ObstetriciaFrancisca Isabel Ramos OrtegaNoch keine Bewertungen
- Hemorragia y Hematoma PuerperalDokument26 SeitenHemorragia y Hematoma Puerperalwaltersantos9080% (5)
- Incontinencia UrinariaDokument80 SeitenIncontinencia UrinariamancardozoNoch keine Bewertungen
- Inducción y Conducción Del PartoDokument9 SeitenInducción y Conducción Del Partonajidaelmasri100% (1)
- Cancer Gastrico FarahDokument13 SeitenCancer Gastrico FarahFarah Zarzar AnguloNoch keine Bewertungen
- Desproporcion FetopelvicaDokument50 SeitenDesproporcion FetopelvicaElizabeth Silva G100% (2)
- Shock en ObstetriciaDokument36 SeitenShock en ObstetriciaJoselyn Ramirez VargasNoch keine Bewertungen
- Casos PDFDokument472 SeitenCasos PDFLizbethMilagrosNoch keine Bewertungen
- Clasificación de BockusDokument3 SeitenClasificación de BockusRicardo Haro100% (1)
- Insuficiencia Venosa Cronica en Miembros InferioresDokument19 SeitenInsuficiencia Venosa Cronica en Miembros InferioresNatasha Morales100% (1)
- Semiologia ObstetricaDokument31 SeitenSemiologia ObstetricaAlheni Fabiola Miranda GomezNoch keine Bewertungen
- Amenaza de Parto PreterminoDokument42 SeitenAmenaza de Parto PreterminoJavier Manuel Escobedo Calderón100% (1)
- Variedades de Posición de La PresentaciónDokument28 SeitenVariedades de Posición de La PresentaciónMer SequeiraNoch keine Bewertungen
- Ecografia Ginecológica 212Dokument11 SeitenEcografia Ginecológica 212Maria Lourddes Garcia LopezNoch keine Bewertungen
- Rciu GabbeDokument36 SeitenRciu GabbeJuan Camilo Vergara100% (1)
- Lesiones Premalignas y Malignas Del Cuerpo UterinoDokument20 SeitenLesiones Premalignas y Malignas Del Cuerpo UterinoRonald Arenas RamirezNoch keine Bewertungen
- Cáncer de Cuello Uterino DX y TX Dr. Hernández 2019Dokument130 SeitenCáncer de Cuello Uterino DX y TX Dr. Hernández 2019Pedro Hernandez Moron100% (2)
- Varicocele e InfertilidadDokument21 SeitenVaricocele e InfertilidadBárbara Pinto PadillaNoch keine Bewertungen
- Ligamentos Del UteroDokument3 SeitenLigamentos Del UteroSamanthaNoch keine Bewertungen
- Gasometría Arteria - UpToDateDokument38 SeitenGasometría Arteria - UpToDatePORTUGAL ESTIVAREZ KEYSI ROSENoch keine Bewertungen
- Contusion PulmonarDokument3 SeitenContusion PulmonarSharow RojasNoch keine Bewertungen
- Manual Espirometria ALAT 2007Dokument76 SeitenManual Espirometria ALAT 2007Edwin Cv100% (3)
- Compresion Manual de La AortaDokument10 SeitenCompresion Manual de La Aortaliz_ast_cb100% (1)
- Criterios IOTADokument7 SeitenCriterios IOTAronald_ar100% (1)
- Caso Problema 7Dokument5 SeitenCaso Problema 7Jessa NoemiNoch keine Bewertungen
- Guias nenonatologíaHLS 2019 PDFDokument474 SeitenGuias nenonatologíaHLS 2019 PDFvickineNoch keine Bewertungen
- Sangrado Uterino AnormalDokument4 SeitenSangrado Uterino AnormalCamila Espinoza BarrazaNoch keine Bewertungen
- Infecciones Urinarias Durante El EmbarazoDokument9 SeitenInfecciones Urinarias Durante El EmbarazoYuliana Alexandra LopezNoch keine Bewertungen
- Desgarros PerinealesDokument36 SeitenDesgarros PerinealesMiguel Angel Martinez LópezNoch keine Bewertungen
- 10 Tecnica Quirurgica de La Cesarea PDFDokument38 Seiten10 Tecnica Quirurgica de La Cesarea PDFgregory paulino100% (1)
- OligoamniosDokument14 SeitenOligoamniosCristhian Santos Bejar0% (1)
- Cirugía hepatobiliar en Colombia: Perspectiva para no olvidar la historiaVon EverandCirugía hepatobiliar en Colombia: Perspectiva para no olvidar la historiaNoch keine Bewertungen
- Columna Estratigrafica de Cajamarca 1Dokument1 SeiteColumna Estratigrafica de Cajamarca 1Anonymous wze4zU0% (1)
- Caolin Ceramica y Vidrio PDFDokument14 SeitenCaolin Ceramica y Vidrio PDFTorrico BorjaNoch keine Bewertungen
- FT Logic LD5 111217Dokument2 SeitenFT Logic LD5 111217Anonymous wze4zUNoch keine Bewertungen
- Letras de Canciones en Ingles - 01Dokument1 SeiteLetras de Canciones en Ingles - 01Anonymous wze4zUNoch keine Bewertungen
- Brochure LaboratorioDokument2 SeitenBrochure LaboratorioAnonymous wze4zU100% (1)
- Protector Coxal de OroDokument2 SeitenProtector Coxal de OroAnonymous wze4zUNoch keine Bewertungen
- Frases Comunes InglesDokument16 SeitenFrases Comunes InglesAnonymous wze4zUNoch keine Bewertungen
- Acopio de Carbon PDFDokument88 SeitenAcopio de Carbon PDFAnonymous wze4zUNoch keine Bewertungen
- Brochure DIADokument16 SeitenBrochure DIAAnonymous wze4zUNoch keine Bewertungen
- Reporte de Sunset Cove BolsaDokument2 SeitenReporte de Sunset Cove BolsaAnonymous wze4zUNoch keine Bewertungen
- Reporte Sunset Cove Bolsa PDFDokument6 SeitenReporte Sunset Cove Bolsa PDFAnonymous wze4zUNoch keine Bewertungen
- Division de Polinomios Metodo de HornerDokument5 SeitenDivision de Polinomios Metodo de HornerElber RabanalNoch keine Bewertungen
- Normalidad y Anormalidad Marco Aurelio DenegriDokument46 SeitenNormalidad y Anormalidad Marco Aurelio DenegriAnonymous wze4zU100% (6)
- HEMONEUMOTORAXDokument3 SeitenHEMONEUMOTORAXDahiana L. NúñezNoch keine Bewertungen
- ElectromedicinaDokument5 SeitenElectromedicinaJesús Percusión MarcanoNoch keine Bewertungen
- Alimentacion Saludable en Tiempos de PandemiaDokument4 SeitenAlimentacion Saludable en Tiempos de Pandemiasiara paezNoch keine Bewertungen
- Luis HernandezDokument3 SeitenLuis HernandezMonica DPNoch keine Bewertungen
- Northwestern Medicine Diabetes Hipoglicemia HiperglicemiaDokument4 SeitenNorthwestern Medicine Diabetes Hipoglicemia HiperglicemiaChon ChiNoch keine Bewertungen
- Pasantias Yosman y MassielDokument66 SeitenPasantias Yosman y MassielDigna RicoNoch keine Bewertungen
- Directorio Salud Mental Prevencion Suicidio MinsaludDokument20 SeitenDirectorio Salud Mental Prevencion Suicidio MinsaludMonikNoch keine Bewertungen
- Farmacia YuliskaDokument3 SeitenFarmacia YuliskaAlfonso SanchezNoch keine Bewertungen
- AdiccionesDokument15 SeitenAdiccionesjuan esteban uran marinNoch keine Bewertungen
- Contenido - Informe Anual HSEDokument5 SeitenContenido - Informe Anual HSEPILAR AMÉZQUITA100% (1)
- Polipos y NodulosDokument12 SeitenPolipos y NodulosYariatna OteroNoch keine Bewertungen
- Anamnesis TelDokument3 SeitenAnamnesis TelElizabeth Paredes LazoNoch keine Bewertungen
- Hemorragia Postparto Precoz MANEJO OBSTÉTRICODokument36 SeitenHemorragia Postparto Precoz MANEJO OBSTÉTRICOcamilaNoch keine Bewertungen
- SO-G11 Guía SVE para El Control Del Riesgo Biológico - PuDokument12 SeitenSO-G11 Guía SVE para El Control Del Riesgo Biológico - Puadric181Noch keine Bewertungen
- Protocolo de Investigacion: Tema: Ausencia de Dientes PorDokument10 SeitenProtocolo de Investigacion: Tema: Ausencia de Dientes Porana paula mendoza rodriguezNoch keine Bewertungen
- Asis Saman 2021 CulminadoDokument25 SeitenAsis Saman 2021 CulminadoJulio HernándezNoch keine Bewertungen
- Carta de Comprimiso - Maria Fernanda GallegoDokument2 SeitenCarta de Comprimiso - Maria Fernanda GallegoJordy Elian Mosquera HernandezNoch keine Bewertungen
- Manual Atencion Parto ExtrahospitalarioDokument81 SeitenManual Atencion Parto ExtrahospitalarioOihane Ml100% (2)
- Medicina LegalDokument35 SeitenMedicina LegalDayana Soto RemigioNoch keine Bewertungen
- 6 (1y2) - Respuestas ClínicasDokument34 Seiten6 (1y2) - Respuestas ClínicasJOSHUA O BRYAN HURTADO VIVARNoch keine Bewertungen
- Folleto de Realización de Discusión DiagnosticaDokument16 SeitenFolleto de Realización de Discusión DiagnosticaDaniel Alejandro Vazquez AriasNoch keine Bewertungen
- En EsDokument4 SeitenEn EsAndres VallejoNoch keine Bewertungen
- TAES - Comunitario - Módulo - IVDokument30 SeitenTAES - Comunitario - Módulo - IVPEDRO TORONoch keine Bewertungen
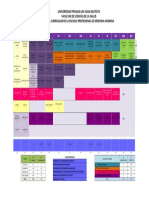
- Malla Curricular Medicina Humana UPSJBDokument1 SeiteMalla Curricular Medicina Humana UPSJBBianca Cavero100% (1)
- Mbe 2Dokument7 SeitenMbe 2alvaroNoch keine Bewertungen
- Ensayo AntraxDokument3 SeitenEnsayo AntraxGustavo MurgaNoch keine Bewertungen
- Trastornos Neuropsiquiátricos Por Trauma CraneoencefálicoDokument31 SeitenTrastornos Neuropsiquiátricos Por Trauma CraneoencefálicoTattuSalgadoNoch keine Bewertungen
- 2021-1 Casos Integradores 3 Fibrosis Pulmonar IdiopaticaDokument31 Seiten2021-1 Casos Integradores 3 Fibrosis Pulmonar IdiopaticaCAROLINA CHUMACERO BERMEONoch keine Bewertungen
- TRIAGE para Imprimir de LuzDokument6 SeitenTRIAGE para Imprimir de LuzLuz Dany Arevalo EspinozaNoch keine Bewertungen
- Pediatria Fisioterapia Respiratoria PracticaDokument6 SeitenPediatria Fisioterapia Respiratoria PracticaDianNoch keine Bewertungen