Das könnte Ihnen auch gefallen
- Student Precepting Log Liver TransplantDokument1 SeiteStudent Precepting Log Liver Transplantapi-405403250Noch keine Bewertungen
- Teaching PhilosophyDokument2 SeitenTeaching Philosophyapi-405403250Noch keine Bewertungen
- Bugs Drugs Inservice 9-17-17Dokument19 SeitenBugs Drugs Inservice 9-17-17api-405403250Noch keine Bewertungen
- Topic Discussion 5 - StagingDokument5 SeitenTopic Discussion 5 - Stagingapi-405403250Noch keine Bewertungen
- Topic Discussion 3 - HCV Presentation and Disease ProgressionDokument3 SeitenTopic Discussion 3 - HCV Presentation and Disease Progressionapi-405403250Noch keine Bewertungen
- Topic Discussion 4 - TreatmentDokument7 SeitenTopic Discussion 4 - Treatmentapi-405403250Noch keine Bewertungen
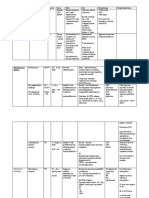
- Antifungal Drug TableDokument2 SeitenAntifungal Drug Tableapi-405403250Noch keine Bewertungen
- Immunosuppressive Agetns in Sot NotesDokument2 SeitenImmunosuppressive Agetns in Sot Notesapi-405403250Noch keine Bewertungen
- Topic Discussion 2 - LabsDokument2 SeitenTopic Discussion 2 - Labsapi-405403250Noch keine Bewertungen
- Endemic Fungi Handout BlankDokument4 SeitenEndemic Fungi Handout Blankapi-405403250Noch keine Bewertungen
- ImmunosuppressantsDokument3 SeitenImmunosuppressantsapi-405403250Noch keine Bewertungen
- 2016 Teaching Experience LogDokument2 Seiten2016 Teaching Experience Logapi-405403250Noch keine Bewertungen
- Technician Lecture 2-26 Choward FinalDokument64 SeitenTechnician Lecture 2-26 Choward Finalapi-405403250Noch keine Bewertungen
- January 2012: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDokument13 SeitenJanuary 2012: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayBobby ParksNoch keine Bewertungen
- Lifecare Inservice CH 8-2017 PDFDokument49 SeitenLifecare Inservice CH 8-2017 PDFapi-405403250Noch keine Bewertungen
- FQ Id Case ConferenceDokument50 SeitenFQ Id Case Conferenceapi-405403250Noch keine Bewertungen
- Howard Neurology Ce FinalDokument65 SeitenHoward Neurology Ce Finalapi-405403250Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Chapter 18 Path and Lab Set BDokument4 SeitenChapter 18 Path and Lab Set BBernard Paul Guinto0% (1)
- Mutations in Myostatin (GDF8) in Double-Muscled Belgian Blue and Piedmontese CattleDokument8 SeitenMutations in Myostatin (GDF8) in Double-Muscled Belgian Blue and Piedmontese Cattlejose noel garcia perezNoch keine Bewertungen
- Veterinary Microbiology: S.C. BishopDokument6 SeitenVeterinary Microbiology: S.C. BishopMuralidhar MettaNoch keine Bewertungen
- Medication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1Dokument77 SeitenMedication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1doodrillNoch keine Bewertungen
- Blood Transfusion Policy 6.3Dokument90 SeitenBlood Transfusion Policy 6.3raNoch keine Bewertungen
- Dna RepairDokument20 SeitenDna RepairEaron Van JaboliNoch keine Bewertungen
- Anal Sex: An 'Extraordinary Taboo': BYLINE: Melby, Todd SECTION: Pg. 1 Vol. 41 No. 11 LENGTH: 2091 WordsDokument7 SeitenAnal Sex: An 'Extraordinary Taboo': BYLINE: Melby, Todd SECTION: Pg. 1 Vol. 41 No. 11 LENGTH: 2091 WordsMichael GarciaNoch keine Bewertungen
- Report Hand Sanitizers Report 1 JuneDokument58 SeitenReport Hand Sanitizers Report 1 JuneMarienNoch keine Bewertungen
- Lymphatic System TransDokument17 SeitenLymphatic System TransRheeanne AmilasanNoch keine Bewertungen
- 2nd Sem Q1 Week 1 Lesson 1 Genetic EngineeringDokument42 Seiten2nd Sem Q1 Week 1 Lesson 1 Genetic Engineeringayesha iris matillaNoch keine Bewertungen
- Welfare of Animals During TransportDokument130 SeitenWelfare of Animals During TransportLeo PerezNoch keine Bewertungen
- Pathway of PulpDokument120 SeitenPathway of PulpTanuj Singh100% (1)
- Week 8 - EctoparasitesDokument57 SeitenWeek 8 - Ectoparasiteshakkam100% (1)
- )Dokument6 Seiten)nuraninarunNoch keine Bewertungen
- Pediatric Hematology Oncology CaseDokument107 SeitenPediatric Hematology Oncology CaseSayyed Ahmad KhursheedNoch keine Bewertungen
- Pretransfusion or Compatibility Testing: NotesDokument7 SeitenPretransfusion or Compatibility Testing: NotesABHINABA GUPTANoch keine Bewertungen
- Disseminated Intravascular CoagulationDokument2 SeitenDisseminated Intravascular CoagulationVince100% (1)
- The Ocular Surface: Maria Markoulli, Judith Flanagan, Shyam Sunder Tummanapalli, Jenny Wu, Mark WillcoxDokument13 SeitenThe Ocular Surface: Maria Markoulli, Judith Flanagan, Shyam Sunder Tummanapalli, Jenny Wu, Mark Willcoxanka_mihaelaNoch keine Bewertungen
- Prokaryotic and Eukaryotic Cells: Two Types of CellsDokument8 SeitenProkaryotic and Eukaryotic Cells: Two Types of CellsMarcy BoralNoch keine Bewertungen
- NIC Health & Safety StandardsDokument3 SeitenNIC Health & Safety StandardsRochelle AngelinaNoch keine Bewertungen
- Gastroeneteritis - Pediatrics (Nelson's)Dokument20 SeitenGastroeneteritis - Pediatrics (Nelson's)Itharshan IndreswaranNoch keine Bewertungen
- "Health Is Wealth": Sickness Causes Remedy Dosage AsthmaDokument18 Seiten"Health Is Wealth": Sickness Causes Remedy Dosage AsthmaYufemo Silvie Epse AloniNoch keine Bewertungen
- DrugsDokument56 SeitenDrugssheela100% (1)
- Summary of Recent Significant Findings in ME-CFS Research - Updated February 2019 PDFDokument21 SeitenSummary of Recent Significant Findings in ME-CFS Research - Updated February 2019 PDFEmilie ChateletNoch keine Bewertungen
- Gardnerella VaginalisDokument12 SeitenGardnerella VaginalisChristian John DelaCruz MolinoNoch keine Bewertungen
- HumaCount 5D ENDokument8 SeitenHumaCount 5D ENAhmed MoeenNoch keine Bewertungen
- JanaDixon PINEAL - OSSIFICATION - PDF PDFDokument22 SeitenJanaDixon PINEAL - OSSIFICATION - PDF PDFefedezeta100% (1)
- Elisa TestDokument11 SeitenElisa Testtofan widyaNoch keine Bewertungen
- Labreportnew PDFDokument8 SeitenLabreportnew PDFLuCky100% (1)
- Dr. Diah Rumekti hadiatiAPCGS JogjaDokument25 SeitenDr. Diah Rumekti hadiatiAPCGS JogjacirererereNoch keine Bewertungen