Das könnte Ihnen auch gefallen
- Genetics of Ectopia Lentis - Sadiq.2013Dokument8 SeitenGenetics of Ectopia Lentis - Sadiq.2013Surya Nirmala DewiNoch keine Bewertungen
- Lens and CataractDokument31 SeitenLens and CataractReinhard TuerahNoch keine Bewertungen
- Pseudoexfoliation Syndrome in Cataract Surgery: Ophthalmic PearlsDokument3 SeitenPseudoexfoliation Syndrome in Cataract Surgery: Ophthalmic PearlsgeorginaNoch keine Bewertungen
- Artigo Management of Ectopia - Neely - 2001Dokument7 SeitenArtigo Management of Ectopia - Neely - 2001Giovanna SoaresNoch keine Bewertungen
- Homoeopathy Treatment of Vitreous OpacitiesDokument4 SeitenHomoeopathy Treatment of Vitreous OpacitiesVitorio VenturiniNoch keine Bewertungen
- Racgp Floaters and Flashes OpthalmologyDokument3 SeitenRacgp Floaters and Flashes OpthalmologyBeaulah HunidzariraNoch keine Bewertungen
- March 2019 Ophthalmic PearlsDokument2 SeitenMarch 2019 Ophthalmic PearlsApps OmNoch keine Bewertungen
- Subluksasi LensaDokument12 SeitenSubluksasi LensaIta RositaNoch keine Bewertungen
- ProP - Differentiating Nuclear Sclerosis From CataractsDokument6 SeitenProP - Differentiating Nuclear Sclerosis From CataractsDita TaepangNoch keine Bewertungen
- Amaya2003 PDFDokument20 SeitenAmaya2003 PDFasfwegereNoch keine Bewertungen
- Ocular Features of Marfan Syndrome: Diagnosis and ManagementDokument4 SeitenOcular Features of Marfan Syndrome: Diagnosis and ManagementmongiiiNoch keine Bewertungen
- Miopi X Katarak 4Dokument5 SeitenMiopi X Katarak 4Melati Nurul UtamiNoch keine Bewertungen
- Cataract Surgery in Eyes With Pseudoexfoliation Pex Syndrome 2155 9570 S1 009 PDFDokument5 SeitenCataract Surgery in Eyes With Pseudoexfoliation Pex Syndrome 2155 9570 S1 009 PDFismihabNoch keine Bewertungen
- Lens and Cataract Group 7Dokument66 SeitenLens and Cataract Group 7Symon MillarNoch keine Bewertungen
- Background: Ectopia Lentis. Dislocated Traumatic Lens (Cataract)Dokument7 SeitenBackground: Ectopia Lentis. Dislocated Traumatic Lens (Cataract)Muhammad Khairul AfifNoch keine Bewertungen
- Literature Review 2.1. Anatomy of The LensDokument9 SeitenLiterature Review 2.1. Anatomy of The LensIka KrastanayaNoch keine Bewertungen
- Intraocular Lens Subluxation in Marfan SyndromeDokument3 SeitenIntraocular Lens Subluxation in Marfan SyndromeSusPa NarahaNoch keine Bewertungen
- Pupil Capture of Intraocular Lens in Vitrectomized Eye With Primary Pigment Dispersion SyndromeDokument2 SeitenPupil Capture of Intraocular Lens in Vitrectomized Eye With Primary Pigment Dispersion SyndromeHuang WanjingNoch keine Bewertungen
- Management of Corneal Abrasions: STEPHEN A. WILSON, M.D., and ALLEN LAST, M.D., University of Pittsburgh Medical CenterDokument6 SeitenManagement of Corneal Abrasions: STEPHEN A. WILSON, M.D., and ALLEN LAST, M.D., University of Pittsburgh Medical CenterGokull ShautriNoch keine Bewertungen
- Retinal Detachment: PathogenesisDokument8 SeitenRetinal Detachment: PathogenesisRashellya RasyidaNoch keine Bewertungen
- Corneal Dystrophies: Retinal DetachmentDokument5 SeitenCorneal Dystrophies: Retinal DetachmentCake ManNoch keine Bewertungen
- Review: Pathogenesis of Rhegmatogenous Retinal Detachment Predisposing Anatomy and Cell BiologyDokument12 SeitenReview: Pathogenesis of Rhegmatogenous Retinal Detachment Predisposing Anatomy and Cell BiologyFathirNoch keine Bewertungen
- Other Anterior Segment Complications Part 2. AyuDokument21 SeitenOther Anterior Segment Complications Part 2. AyuAndi Ayu LestariNoch keine Bewertungen
- Vitreous FloatersDokument35 SeitenVitreous FloatersnadiasalimaNoch keine Bewertungen
- Mac HoleDokument21 SeitenMac HoleSwati RamtekeNoch keine Bewertungen
- February 2016 Ophthalmic Pearls PDFDokument3 SeitenFebruary 2016 Ophthalmic Pearls PDFIndah IndrianiNoch keine Bewertungen
- Lens Biology: Development and Human CataractogenesisDokument6 SeitenLens Biology: Development and Human CataractogenesismeliabudiNoch keine Bewertungen
- Bo 402 (32301721022)Dokument8 SeitenBo 402 (32301721022)AvinabaNoch keine Bewertungen
- Polar CataractDokument7 SeitenPolar Cataractjennifersteffi22Noch keine Bewertungen
- Katowitz2009Dokument13 SeitenKatowitz2009Priscilla GeraldineNoch keine Bewertungen
- 43820-Article Text-41628-1-10-20090630 PDFDokument5 Seiten43820-Article Text-41628-1-10-20090630 PDFDr. Candy Delos Reyes-BarluadoNoch keine Bewertungen
- Md2024 Corneal DiseaseDokument3 SeitenMd2024 Corneal DiseaseRohanNoch keine Bewertungen
- Corneal Opacities in The Neonate: Education GapsDokument10 SeitenCorneal Opacities in The Neonate: Education GapsOMAR ORENoch keine Bewertungen
- Human Malformations - 09 - EyeDokument29 SeitenHuman Malformations - 09 - EyeAhmed H. Ali ElbestaweyNoch keine Bewertungen
- Terminology: Nuclear Sclerotic CataractsDokument4 SeitenTerminology: Nuclear Sclerotic CataractsBenjamin NgNoch keine Bewertungen
- Corneal Dystrophies: Retinal DetachmentDokument6 SeitenCorneal Dystrophies: Retinal DetachmentMarissa AsimNoch keine Bewertungen
- New Management Strategies For Ectopia LentisDokument14 SeitenNew Management Strategies For Ectopia LentisximoNoch keine Bewertungen
- Pediatric Neuro Ophthalmology, Lim, Curr Opin Ophthalmol, 2004Dokument7 SeitenPediatric Neuro Ophthalmology, Lim, Curr Opin Ophthalmol, 2004Evelyn SepulvedaNoch keine Bewertungen
- Eor CataractDokument3 SeitenEor CataractDaneva ReyesNoch keine Bewertungen
- Moduleblock Xiii 2.2 Hazy VisionDokument13 SeitenModuleblock Xiii 2.2 Hazy VisionPrincess Noreen SavellanoNoch keine Bewertungen
- Globe Luxation, Complex Eyelid PDFDokument3 SeitenGlobe Luxation, Complex Eyelid PDFNisaNoch keine Bewertungen
- Cataract Aiims Aipgmee Pgi Jipmer DNB McqsDokument41 SeitenCataract Aiims Aipgmee Pgi Jipmer DNB Mcqsजेनिश न्यौपानेNoch keine Bewertungen
- Childhood Cataracts and Other JadiDokument49 SeitenChildhood Cataracts and Other JadiSania NadianisaNoch keine Bewertungen
- Case Report - Traumatic CataractDokument4 SeitenCase Report - Traumatic CataractMaria LarasatiNoch keine Bewertungen
- Jewel June Gutierrez N-31 Rosejel Mae Lagura Senile Cataract IDokument4 SeitenJewel June Gutierrez N-31 Rosejel Mae Lagura Senile Cataract IJewel GutierrezNoch keine Bewertungen
- Retinal DetachmentDokument3 SeitenRetinal DetachmentzeejayNoch keine Bewertungen
- Cataract PPT FinalDokument37 SeitenCataract PPT FinalSibi John91% (22)
- Congenital Optic Nerve Anomalies: Nandini Singh S.NO: 63 Roll No:68Dokument54 SeitenCongenital Optic Nerve Anomalies: Nandini Singh S.NO: 63 Roll No:68nandini singhNoch keine Bewertungen
- What Are Refractive Errors?Dokument20 SeitenWhat Are Refractive Errors?Eduardo Niepes Jr.Noch keine Bewertungen
- Course 7 I, IIDokument17 SeitenCourse 7 I, IItaliya. shvetzNoch keine Bewertungen
- Imaging of The CorneaDokument6 SeitenImaging of The CorneaRael Rodrigues Dos SantosNoch keine Bewertungen
- Management of DiplopiaDokument5 SeitenManagement of Diplopiacahyati syhrilNoch keine Bewertungen
- MainDokument7 SeitenMainSyeda F AmbreenNoch keine Bewertungen
- Corneal Abrasion: BackgroundDokument9 SeitenCorneal Abrasion: Backgroundmd_putra10Noch keine Bewertungen
- Cataract NotesDokument4 SeitenCataract NotesJeremy LauNoch keine Bewertungen
- Management of Retinal Detachment: A Guide For Non-OphthalmologistsDokument6 SeitenManagement of Retinal Detachment: A Guide For Non-OphthalmologistsadriantiariNoch keine Bewertungen
- Separation Astigmatism,: Ectopia LentisDokument2 SeitenSeparation Astigmatism,: Ectopia LentisRizkia Retno DwiningrumNoch keine Bewertungen
- Congenital Disorders of The CorneaDokument100 SeitenCongenital Disorders of The Corneaeyemd_in_trainingNoch keine Bewertungen
- Abrasi KorneaDokument4 SeitenAbrasi KorneaHanaNoch keine Bewertungen
- WHLP12 Quarter 1Dokument8 SeitenWHLP12 Quarter 1rhaineNoch keine Bewertungen
- Chapter End Stop SignsDokument4 SeitenChapter End Stop Signsapi-307327939Noch keine Bewertungen
- GUIA Inglés 2 ADV ExtraordinarioDokument2 SeitenGUIA Inglés 2 ADV ExtraordinarioPaulo GallegosNoch keine Bewertungen
- Test Bank For Criminal Law 10th Edition Joycelyn M Pollock DownloadDokument36 SeitenTest Bank For Criminal Law 10th Edition Joycelyn M Pollock Downloadfisccarriage.z8yu4e100% (40)
- Lister LPW Marine Spec SheetDokument2 SeitenLister LPW Marine Spec SheetMartyn PitmanNoch keine Bewertungen
- Reviewer For Inventions and Filipino InventorsDokument10 SeitenReviewer For Inventions and Filipino InventorsAila AganaNoch keine Bewertungen
- Designs Catalogue With Basic Drawings - 7th Dec 21 1Dokument29 SeitenDesigns Catalogue With Basic Drawings - 7th Dec 21 1Ibrar HussainNoch keine Bewertungen
- JaundiceDokument9 SeitenJaundiceJean Pierre LapennaNoch keine Bewertungen
- Evaporative Emission Control System: GeneralDokument5 SeitenEvaporative Emission Control System: Generalbob loblawNoch keine Bewertungen
- Chapter 12 PDFDokument50 SeitenChapter 12 PDFNaveen DharavathNoch keine Bewertungen
- Format. Hum - The Right To Privacy Is Protected As An Intrinsic Part of The Right To Life and Personal Liberty Under Article 21 of The Constitution of India An EvaluationDokument12 SeitenFormat. Hum - The Right To Privacy Is Protected As An Intrinsic Part of The Right To Life and Personal Liberty Under Article 21 of The Constitution of India An EvaluationImpact JournalsNoch keine Bewertungen
- Difference Between Executor Exe ServiceDokument4 SeitenDifference Between Executor Exe ServiceMadura NattuduraiNoch keine Bewertungen
- Columna de Concreto 1 DanielDokument3 SeitenColumna de Concreto 1 Danielpradeepjoshi007Noch keine Bewertungen
- Construction Equipment GuideDokument17 SeitenConstruction Equipment GuideSamuel Espartero100% (3)
- G Schock G-2210 ManualDokument2 SeitenG Schock G-2210 ManualcaquirinoNoch keine Bewertungen
- Dangerous Prohibited Goods Packaging Post GuideDokument66 SeitenDangerous Prohibited Goods Packaging Post Guidetonyd3Noch keine Bewertungen
- Paper171 I.banuDokument6 SeitenPaper171 I.banuIoan-Viorel BanuNoch keine Bewertungen
- BEEF Scholars Merit List Selected On The Basis of 1st Semester GPA of Course Work, Enrolled in BUITEMS QTADokument6 SeitenBEEF Scholars Merit List Selected On The Basis of 1st Semester GPA of Course Work, Enrolled in BUITEMS QTAKhan QuettaNoch keine Bewertungen
- Remote Digital Input (Rdi-32Xe / Rdi-32Axe) : Distributed Processing UnitsDokument2 SeitenRemote Digital Input (Rdi-32Xe / Rdi-32Axe) : Distributed Processing UnitsCHAIRMANNoch keine Bewertungen
- Steel - WikipediaDokument16 SeitenSteel - WikipediaaravindNoch keine Bewertungen
- Methyl Isocyanate (MIC) Rundown & Storage System: The Bhopal Gas Tragedy Technical Series Part 1 of 4Dokument3 SeitenMethyl Isocyanate (MIC) Rundown & Storage System: The Bhopal Gas Tragedy Technical Series Part 1 of 4Jesse Haney IIINoch keine Bewertungen
- Merger of ING Vysya Bank Ltd. With Kotak Mahindra Bank Ltd.Dokument20 SeitenMerger of ING Vysya Bank Ltd. With Kotak Mahindra Bank Ltd.Prasad JoshiNoch keine Bewertungen
- MT-HN-RCTI-13 - Sealing CracksDokument20 SeitenMT-HN-RCTI-13 - Sealing CracksManuela Angulo TrianaNoch keine Bewertungen
- Potch Girls High Newsletter 13 - 25 November 2016Dokument7 SeitenPotch Girls High Newsletter 13 - 25 November 2016madsdalyNoch keine Bewertungen
- Curriculum Cam I 342Dokument5 SeitenCurriculum Cam I 342ricardojrv3258Noch keine Bewertungen
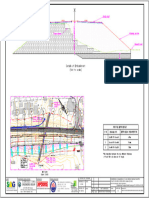
- Sag 011 5267 DSN PW em 24.380 24.520 Ol SG2 100 01Dokument1 SeiteSag 011 5267 DSN PW em 24.380 24.520 Ol SG2 100 01Sanjay SwamiNoch keine Bewertungen
- Cello GRADE 1Dokument11 SeitenCello GRADE 1Paul CortyNoch keine Bewertungen
- SHPB2012 Barras de Cromsteel PDFDokument24 SeitenSHPB2012 Barras de Cromsteel PDFEdgar Rojas EspejoNoch keine Bewertungen
- Math in The Modern World SyllabusDokument4 SeitenMath in The Modern World SyllabusLeandro Amoranto BambeNoch keine Bewertungen
- Chapter6-Sedimentary RocksDokument6 SeitenChapter6-Sedimentary Rockssanaiikhan2020Noch keine Bewertungen