Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Feed Your Flora: How To Promote Healthy Gut Bacteria: Steven Lalevich, RDDokument16 SeitenFeed Your Flora: How To Promote Healthy Gut Bacteria: Steven Lalevich, RDDraganMilenkovićNoch keine Bewertungen
- Health and HygieneDokument20 SeitenHealth and HygieneAnweshaNoch keine Bewertungen
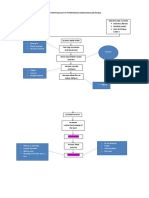
- Pathophysiology of Hypertensive Cardiovascular Disease: Chest Pain Muscle Weakness Shortness of BreathDokument2 SeitenPathophysiology of Hypertensive Cardiovascular Disease: Chest Pain Muscle Weakness Shortness of BreathCyril Jane Caanyagan AcutNoch keine Bewertungen
- IDF Atlas 8e ENDokument157 SeitenIDF Atlas 8e ENAtrik Pristica DianiNoch keine Bewertungen
- Evidence-Based Practice Project: Diabetes Diet Management: Stephanie Green NUR - 590Dokument20 SeitenEvidence-Based Practice Project: Diabetes Diet Management: Stephanie Green NUR - 590dennis ndegeNoch keine Bewertungen
- Nutritional Management in Respiratory DiseasesDokument23 SeitenNutritional Management in Respiratory DiseasesRafia KhalilNoch keine Bewertungen
- LifestyleDokument32 SeitenLifestyleMidz SalipNoch keine Bewertungen
- Bài tập ôn thi giữa học kỳ 1 - Tiếng Anh 7Dokument3 SeitenBài tập ôn thi giữa học kỳ 1 - Tiếng Anh 7Hằng Nguyễn ThịNoch keine Bewertungen
- Stomatitis - AHNDokument22 SeitenStomatitis - AHNZimran SalimNoch keine Bewertungen
- Braden Scale For Predicting Pressure Ulcer RiskDokument1 SeiteBraden Scale For Predicting Pressure Ulcer RiskJian CarloNoch keine Bewertungen
- Essential Readings For IELTSDokument190 SeitenEssential Readings For IELTSEmad Mergan0% (2)
- Mason, John - How To Be A Life Coach-J. Mason (2011) PDFDokument67 SeitenMason, John - How To Be A Life Coach-J. Mason (2011) PDFBrian S. Danzyger100% (1)
- Topic: 6: Food AdditivesDokument6 SeitenTopic: 6: Food Additivesmohammed ansr nmNoch keine Bewertungen
- General Food Distribution. 1Dokument15 SeitenGeneral Food Distribution. 1Hamza JanNoch keine Bewertungen
- Dietary Reference IntakeDokument7 SeitenDietary Reference IntakePolene AfableNoch keine Bewertungen
- Wellness Report by PWCDokument64 SeitenWellness Report by PWCPranav Santurkar100% (1)
- GordonsDokument3 SeitenGordonskrissmeNoch keine Bewertungen
- Fast Food Restaurants Impact On PeopleDokument6 SeitenFast Food Restaurants Impact On PeopleVisa RanicoNoch keine Bewertungen
- Lecture 11 Failure To Thrive (FTT)Dokument25 SeitenLecture 11 Failure To Thrive (FTT)jaish8904100% (2)
- The Cornflake DietDokument8 SeitenThe Cornflake DietSorindah MolinaNoch keine Bewertungen
- Velocity-DIet 3.5.1Dokument75 SeitenVelocity-DIet 3.5.1Yahya Khan100% (1)
- Ncp1 317rle Ronquillo BryanDokument2 SeitenNcp1 317rle Ronquillo BryanPaul AnteNoch keine Bewertungen
- Balanced Diet Grade 2 Comprehension WorksheetDokument2 SeitenBalanced Diet Grade 2 Comprehension WorksheetSaquib.Mahmood100% (7)
- Malnutrition: Intervention Plan Nursing Intervention Method of Nurse Family Contact Resource RequiredDokument1 SeiteMalnutrition: Intervention Plan Nursing Intervention Method of Nurse Family Contact Resource RequiredSareno PJhēaNoch keine Bewertungen
- Tai Sophia Institute Whole Foods Cooking Lab 4 Nutrition 684 Fall 2012 .5 Credits FacultyDokument5 SeitenTai Sophia Institute Whole Foods Cooking Lab 4 Nutrition 684 Fall 2012 .5 Credits Facultyapi-96990759Noch keine Bewertungen
- Clinical PearlsDokument5 SeitenClinical PearlscNoch keine Bewertungen
- AKI in A Neonate: Bharathi BDokument41 SeitenAKI in A Neonate: Bharathi ByaleeeehNoch keine Bewertungen
- Extended Tension - Dave TateDokument12 SeitenExtended Tension - Dave TateHercules Le100% (3)
- BenfotiamineDokument5 SeitenBenfotiaminekether.thipharet5601Noch keine Bewertungen
- BCH301Dokument19 SeitenBCH301yabdallahNoch keine Bewertungen